
Why Don't Statins Cause Dementia?
There's no reason they should, but... why not?

Today’s post is brought to you by my sponsor, Mechanize. They’re hiring junior software engineers at $300K/year base salary.
Spend enough time talking about heart disease online and you will inevitably be confronted with the claim that lowering your cholesterol increases your risk of getting dementia. Why? The reasoning can look like this:
‘Your brain is full of cholesterol. Statins inhibit the cholesterol synthesis enzyme HMG-CoA reductase, and sometimes they enter the brain. Low cholesterol has been associated with dementia in a handful of observational studies. Therefore, LDL lowering with statins or other forms of HMGCR inhibition must deprive the brain of cholesterol and cause dementia.’
And, if someone is reasoning about mechanisms, it can look like this:
‘Statins lower cholesterol levels, leading to a cholesterol shortage in the brain, causing dementia. This happens because cholesterol is needed to support cell membranes in the brain, because it is crucial for myelin, because it’s needed for synapses and synaptic vesicles, and if you lower your cholesterol, all of these things become broken.’
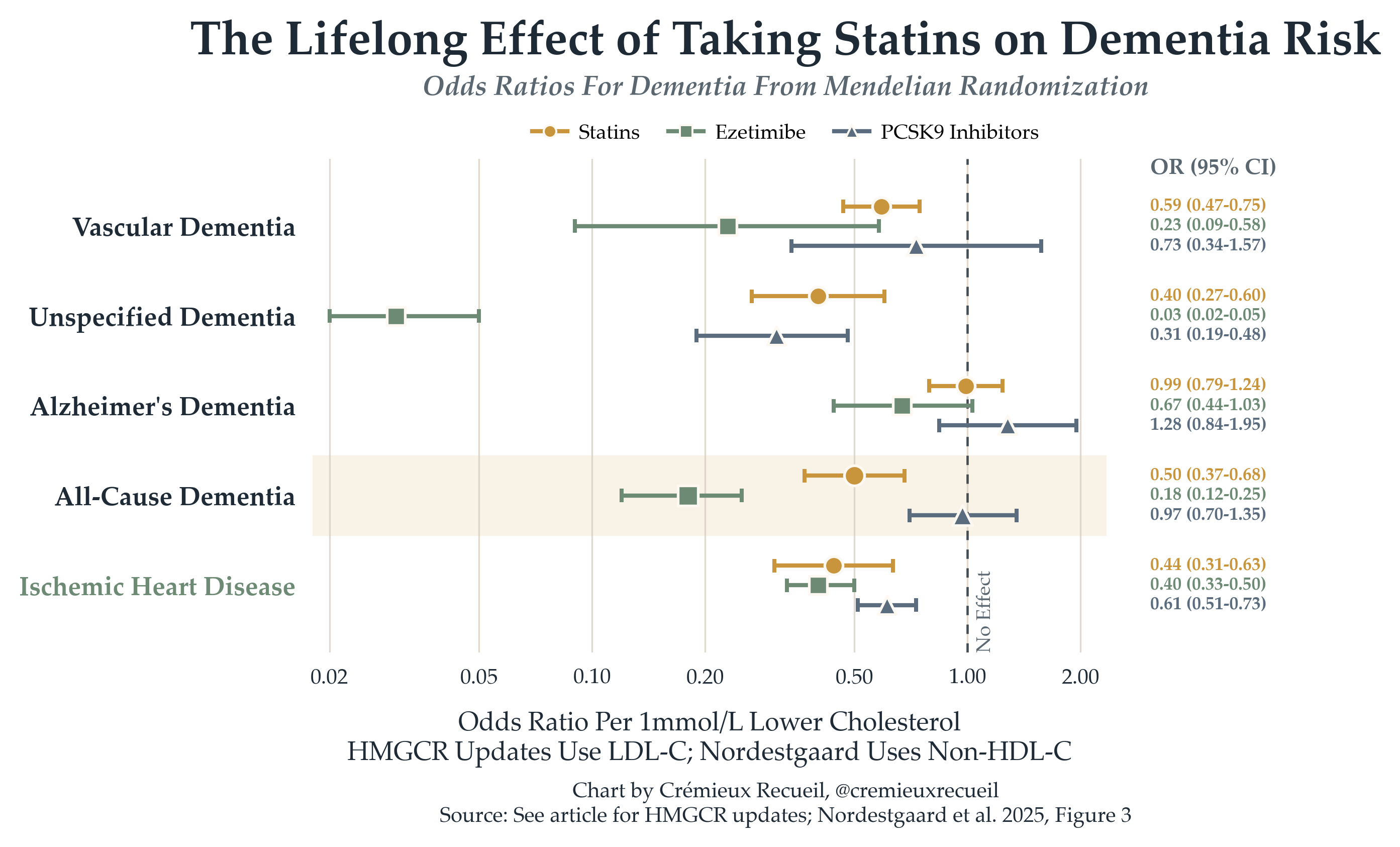
The problem for these and similar theories is that, when you check the data, it doesn’t line up. Mendelian randomization lets us get at the effect of taking statins or other LDL-lowering medications for a person’s whole life—decades of exposure!—and we see basically nothing when it comes to signals of harm. If anything, statins seem good!1

I think these results are only shocking because of semantics. People hear that something called ‘cholesterol’ is involved in the brain and assume that anything that lowers cholesterol must therefore lower it in the brain, depriving the brain of something like a critical nutrient, a requirement to function. But ‘cholesterol’ does not just mean one thing; you do not just have one cholesterol level.
The way statins work is by lowering liver-based cholesterol synthesis, resulting in relatively more hepatic LDL receptor activity, pulling more LDL from the blood, resulting in lower risk of atherosclerosis because of reduced risk of plaque buildup. But the brain, while cholesterol-rich and cholesterol-dependent, does not have its cholesterol supply affected by cholesterol-lowering medication. The main reason for this is the blood-brain barrier (BBB) and the fact that lipoproteins in the blood do not freely enter the brain. Accordingly, to get its cholesterol, the brain has to make and recycle it locally.
Reviews are unequivocal about this:
[C]holesterol in the [central nervous system (CNS)] is almost entirely synthesized within the brain since the BBB prevents any direct transfer of sterols from the blood to the brain, especially when they are contained in lipoprotein particles.
Peripheral (blood) cholesterol and CNS (brain) cholesterol are practically distinct. The brain produces its required cholesterol locally in glial cells, astrocytes, and oligodendrocytes, and it transports within the brain using ApoE-containing lipoprotein-like particles. Where there’s a relationship, it’s primarily through the brain disposing of cholesterol by converting it into 24S-hydroxycholesterol, which crosses the BBB and deposits cholesterol in the bloodstream to bring it to the liver for elimination.2

The National Lipid Association’s (NLA) advice is to lower your cholesterol, for as long as possible, to achieve better heart health.3 This is good advice because, for most people,4 LDL is the key causal factor involved in causing heart disease—specifically, atherosclerotic cardiovascular disease. This is completely unambiguous; with very low LDL, most heart disease goes away.5 And, if you followed this evidence and took the NLA’s advice to heart, you would likely not encounter elevation of dementia risk.
Consider the FOURIER trial. People who attained very low LDL with a PCSK9 inhibitor and a statin didn’t show any worse cognition after 2.2 years. We saw similar results in IMPROVE-IT after six years. Results like these are so often repeated, and so strongly supported by the bulk of trials, prospective cohort studies, and Mendelian randomization evidence that the American College of Cardiology simply maintains that reducing “LDL-C is not associated with cognitive decline or dementia.”6 Full stop.
With that said, LDL lowering does—as we’ve seen—seem to reduce the risk of vascular dementia, and it certainly reduces the risk of stroke. Both of those things either do or can involve serious cognitive impairment, and should for that reason be avoided. If they really cared about cognitive impairment, opponents of statins would be jumping for joy about this. But, revealingly, they remain opposed.
I suspect that the biggest reinforcement for confusion comes from failing to think causally about this issue.
Consider this distinction: someone with very low LDL due to prescribed lipid-lowering drugs is not being cholesterol-starved in the brain. However, someone who has near-zero cholesterol without a medical indication is more likely to have a rare genetic disorder like abetalipoproteinemia or hypobetalipoproteinemia, which comes with impaired fat-soluble vitamin handling and subsequent neurological and eye problems. If you looked at these people in an observational study and didn’t realize their disease state, you might think low LDL causes risks of its own. But, these people are high-risk less due to LDL, and more due to their other issues, which also cause low LDL.7
Additionally, in late life, low cholesterol sometimes indicates illness, frailty, weight loss, inflammation, malnutrition, cancer, or preclinical dementia, even though it’s not its cause. This sort of reverse causation has tricked tons of people into thinking that there are harms. We are lucky, then, that most of the observational evidence seems to be unaffected by these things. Accordingly, if we look at all of it, then we won’t make a big mistake when it comes to LDL, but, two things: first, that’s not always the case; and, second, it’s tempting to look at outlier studies. The best we can do is continue thinking causally, lest we wind up confused.
A message from my sponsor, Mechanize:
We’re hiring software engineers to build environments and evals that frontier AI labs use to train coding agents.
To get a better sense of the work we do, you can check out GBA Eval, where we had models build Game Boy Advance emulators from scratch and scored their performance.
Base pay starts at $300K/year for junior software engineers, with more for senior roles, plus equity and performance bonuses. Apply here.
Other studies have tended to support these findings.
Some oxysterols and dysfunction in the BBB can create interactions between peripheral and brain cholesterol metabolism, but these are not important for most people.
I often get asked some version of the question ‘If we can safely lower [peripheral] LDL to nearly nothing, why does the body produce it anyway?’
The reason is that LDL is not useless per se, even though most cells can regulate their own cholesterol through de novo synthesis, LDL-receptor uptake, storage, and efflux. Similarly, there was, at one point, selection for humans to have an easier time getting fatter, because that was once useful too. Hopefully everyone can agree that being fat is no longer a good thing, as we’re not resource-constrained in our modern environments, and thus it’s unnecessary to store lots of fat. Think similarly for LDL.
Peripheral cholesterol circulation does a few things. Firstly, it moves dietary fat from the gut to muscle and fat tissue. This is how we get chylomicrons. Secondly, it allows the liver to export fuel to peripheral tissues with VLDL, which when progressively emptied of triglyceride becomes IDL and then LDL. Third, it delivers cholesterol when cells want it, for use in cell membranes and precursors for bile acids and steroid hormones. And fourth, it allows retrieving excess cholesterol, because HDL participates in reverse cholesterol transport, where it moves cholesterol from peripheral tissues back to the liver to be reused or excreted in bile and feces.
When LDL is very low, it typically means that LDL particles are being cleared efficiently and are not lingering in the bloodstream. When it’s high, too many apoB lipoprotein particles will be circulating for too long, resulting in more opportunities for them to enter and be retained in artery walls, where they cause damage. A little bit is fine, like how a little bit of fat is necessary; but a lot, for a long time, hurts.
To take the analogy with being fat further, in traditional societies and among chimpanzees, cholesterol levels are typically considerably lower than they are in the modern United States. Likewise, those societies and animals are not as fat as us moderns, on average. When those do have obesity, high LDL, and other issues, they also come with low lifespans or poor monitoring, so no paradoxical ‘unhealthy by modern standards, but nonetheless doing well’ examples have come up with any meaningful level of scrutiny applied to them.



Because of the lack of other mechanisms for plaque buildup.
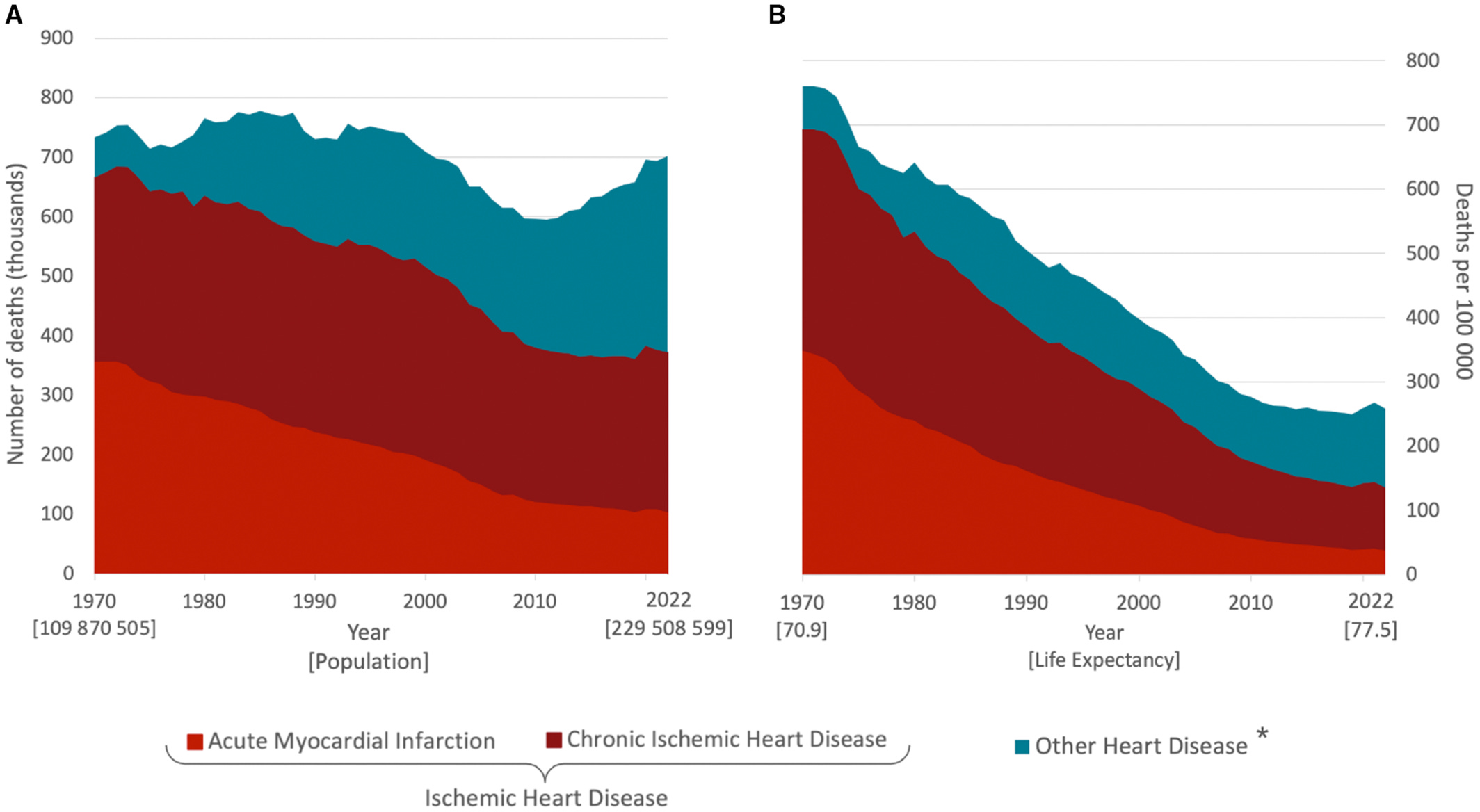
Back in 1970, this would be 91% of all heart disease deaths, and as of 2022, it’s 53%. This leaves behind arrhythmias, heart failures, valve disease, cardiomyopathy, myocarditis, congenital heart disease, hypertensive heart disease, and other conditions, and the main reason for the decline in heart disease is that we’ve substantially tamed the LDL-driven afflictions, even though several factors involved in aggravating it—such as obesity and glycemia—have gotten worse. These other factors are less under the control of the medical system.
This is considerable prima facie evidence that statins have had an amazing impact on cardiovascular health.
If population blood pressure (hypertensive heart disease; heart failure with preserved ejection fracture; atrial fibrillation and many arrhythmias), glycemia, and weight were better controlled, most of the remaining heart disease deaths would likely also disappear. However, this would still not eliminate many cardiomyopathies, myocarditis and pericarditis, congenital heart disease, or many cases of pulmonary heart disease, since they are driven by genetics, viruses and inflammatory disease states, alcohol and drug abuse, chemotherapy, pregnancy, thyroid disease, autoimmune disease, toxins, maternal pregnancy factors, etc.
If you achieve low LDL and are otherwise fit, without major genetic defects, developmental insults, drugs, or serious infection, you are very unlikely to get any form of heart disease.
One common fallback for opponents of statins is to claim that lipophilic statins in particular cross the BBB and are thereby capable of cholesterol-related neurodegeneration. But, for one, we don’t see any evidence of this in large cohort studies. For two, it’s just not clear there’s any harm at all, and there is evidence for benefits to taking lipophilic statins. For three, there shouldn’t be much in the way of effects because lipophilic statins still don’t enter the brain that much, just more than the virtually nonexistent level of penetration from hydrophilic statins. For four, the brain compensates for effects from crossing the BBB. In the main study that’s cited on this, researchers noticed that high-dose simvastatin treatment led to reductions in 24S-hydroxycholesterol, suggestion that the brain was depositing a slightly smaller amount of its produced cholesterol in the blood. The authors suggested this could be a mechanism behind statins defending people from Alzheimer’s. And finally, if you believe there’s a problem, just take/prescribe/recommend/whatever a hydrophilic statin or a different LDL-lowering drug to get LDL down.
We can be sure of this because simple lowering in trials and from drug-like genetic instruments in Mendelian randomization studies shows us as much.
Thank
Excellent breakdown. The blood-brain barrier explanation is what most people making the statin-dementia argument have never encountered. Once you understand that peripheral and brain cholesterol operate as practically separate systems, the whole mechanism falls apart.