
Will Making Your Kids Tall Shorten Their Lives?
Bonus: How to get human growth hormone (HGH) for cheap

Today’s post is brought to you by my sponsor, Mechanize. They’re hiring junior software engineers at $300K/year base salary.
If you just want to skip the data and get down to the part on how to source HGH, click here.



It’s true: people are paying to make their kids taller than they otherwise would’ve been.
And here’s the kicker: it works! By paying a little money up-front, parents are able to make their kids a few inches taller in normal cases and sometimes more than a foot taller in cases where kids are suffering from pathologically low growth hormone levels.
But this raises a nasty question: are these parents murderers? By making their kids taller, are they also raising their risk of different ailments, from cancers to lung tears? Are they giving their kids scoliosis and diabetes in exchange for a handful of precious, socially-valuable inches? After all, it’s common knowledge that taller people—socially advantaged as they are—live shorter lives because they get cancer more often, right?
The answer to that isn’t so clear-cut. Take a look all-cause mortality vs. height:1
But this diagram is based on observational data, it’s basically just a correlation, and we know that what it depicts isn’t likely to be a description of real cause-and-effect.
Consider why people might be very short. Why might a man be 4’10” for example? One prominent reason is dwarfism, which also tends to come with a number of other skeletal and metabolic problems that dispose people to shorter lifespans, above and beyond the effect of just being short. Likewise, consider why someone might be incredibly tall. A person who’s 7’3” is much more likely to be someone who has gigantism, which does indeed make you tall, but also puts you at risk soft tissue swelling, circulatory problems, muscular weakness, and so on.
A more familiar reason for very short stature is osteopenia—age-related bone loss. But if you’re experiencing that, then chances are you have other frailty-disposing comorbidities, and you’re likely to be quite old, with all that entails. To really get at the effect of height on lifespans, we have to go beyond confounded cross-sectional data. But first, we have to ask an even more complicated question:
Are the height gains people experience from taking HGH in their childhood like height in the general population? What if HGH users are gangly, with disproportionate limbs, freakishly widened jaws, and other signs of abnormal growth? Basically: Is it even valid to use data on the heights of normal people to infer something about the eventual heights of HGH users?
First, we need a prior. That prior is going to be “Size matters.” That’s what we’re all going to agree to believe, right now. Size matters. This is a widely accepted view on the risk for cancer: the more cells in the body, the greater the risk of cancer. In fact, this view was articulated in a well-known 2018 paper entitled “Size matters: height, cell number and a person’s risk of cancer”. The key idea from that paper, however, is much older; papers supportive of this case have been published as far back as 1988, more recently in 2013, contemporaneously with “Size matters” in 2018, and plenty of times after the advent of COVID as well. This has been investigated with merely observational and with causally informative methods, and they both agree: more cells, more cancer in humans and in other animals.2
Second, we need to know if HGH-driven growth is isometric or allometric. What this means—and I am slightly misusing these terms—is we need to know if it involves disproportionate growth in some areas compared to others (allometry) or proportionate growth (isometry) when administered throughout regular development.
As it turns out, most literature agrees that the growth is isometric, and that ‘HGH height’ is basically like normal ‘genetic height’. Some data indicates slightly greater renal growth relative to height, and some other data indicates slightly trunk-favoring growth, meaning that sitting height—which is generally a tad more heritable than standing height!—is impacted more by HGH administration. More importantly, compared to their similar-height peers who did not receive HGH, those who did are usually a little lighter, which I’ll return to.
We also have data on what would happen if a person went extremely overboard, because some people are genetically disposed to their bodies doing basically that. In cases with pathologically elevated HGH levels, as in acromegaly, there’s increased epithelial cell proliferation in the colon, leading to an excess of the small, bulgy pouches that happen when intestinal lining pushes through weak parts of the muscular wall when under pressure, and perhaps explaining their higher rates of colorectal and gastric cancer (among a few other elevated types). But even this elevation is slight, and it would be very odd for parents to push their kids this far.
So, to clearly and quickly summarize on the nature of HGH-driven growth as opposed to ‘genetic growth’: given approximate isometry, ‘HGH height’ carries ~70-100% of the cell number-cancer relationship prior, with a mild discount because HGH-treated kids—especially ones starting from a state of HGH deficiency—tend to end up somewhat lighter in terms of both bone and muscle mass. This relative lightness3 has to do with the fact that the HGH-added height is delivered to kids via stimulation of the IGF-1 axis, and for a person at a given ‘genetic height’, that stimulus remains, whereas for ‘HGH height’, it doesn’t. The ‘HGH tall’ kids just keep the height without the rest.
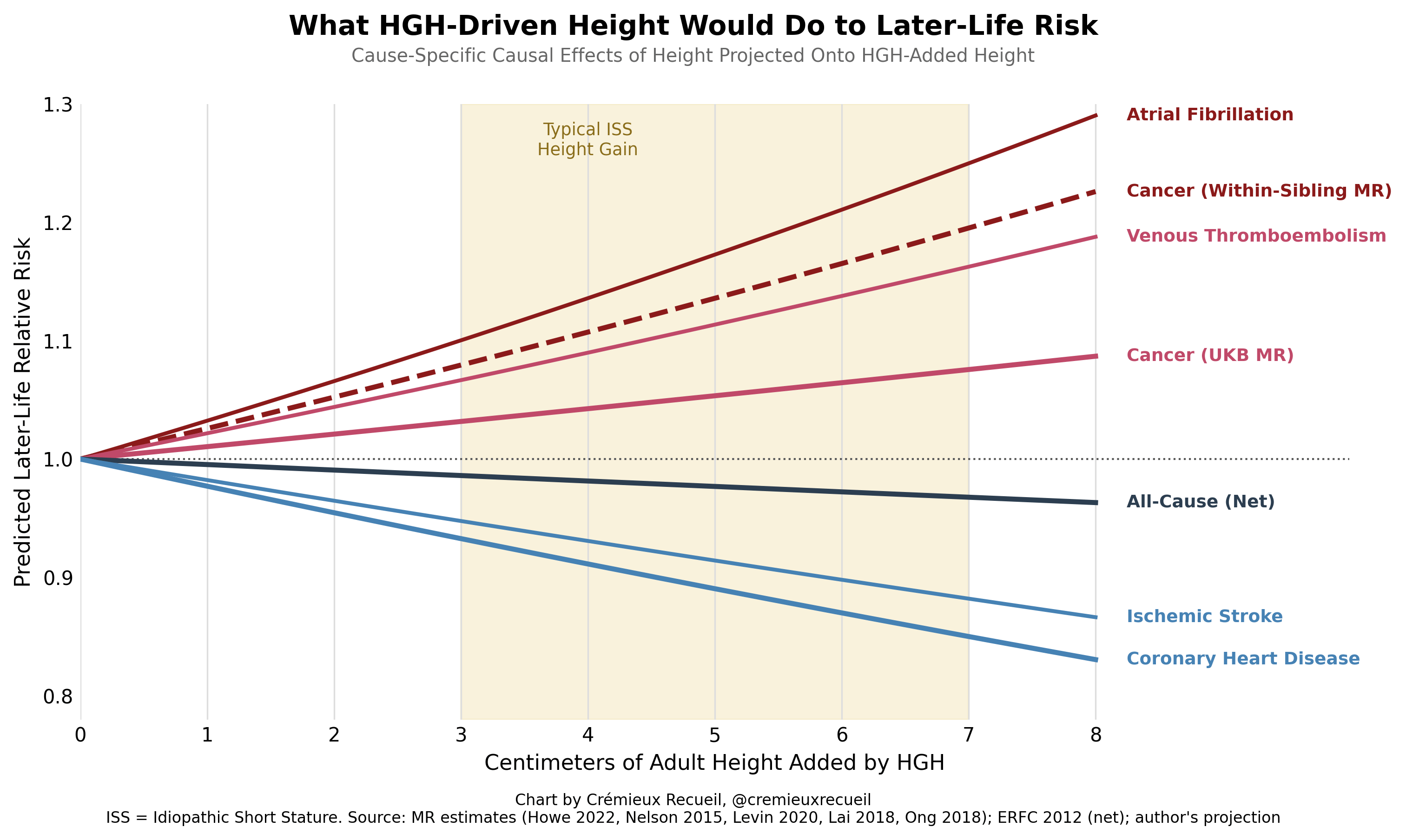
If you throw all of this information together, we end up with a prior that HGH-delivered height will be a little less cancerous than the same ‘genetic height’. But this doesn’t mean adding height is all bad: remember, taller people also end up healthier in other ways. For example, height improves lung function and lipid profiles. On the other side for the heart, it has some unfavorable effects on hemodynamics because it enlarges atria and creates longer venous columns. On net, the causal effect of height on the risk of various conditions and death is… not bad. And we know this because of the wonders of Mendelian Randomization—a method that exploits subtle differences in genetic endowments to estimate the causal effects of things as diverse as having higher or lower cholesterol or being taller or shorter. Take a look at how height affects different conditions:
And if we just want to get at causal curves, well, that’s easy enough! We can that if we sum to get the curves from our Mendelian Randomization! That looks like this:
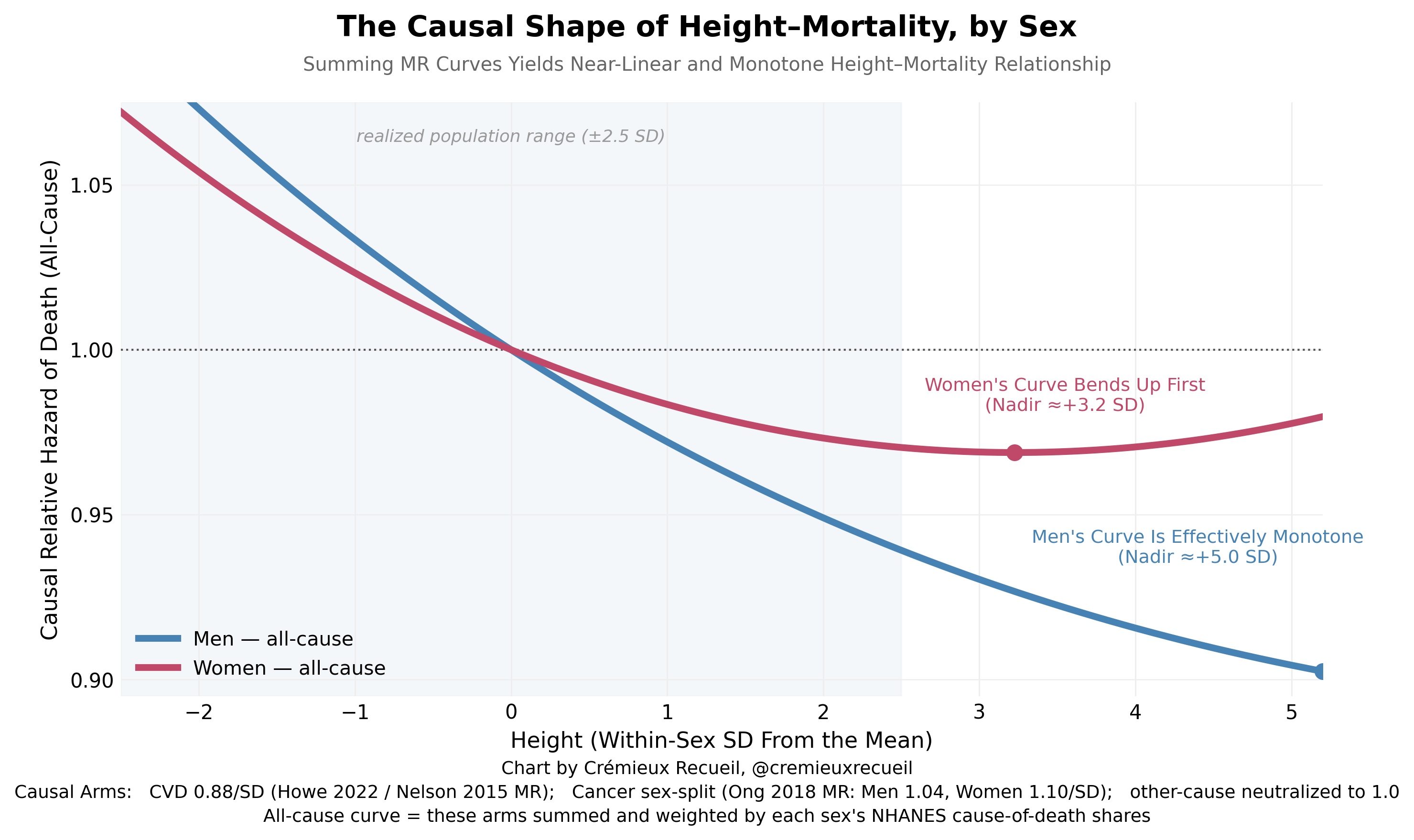
In short, the expected effect of height is on net somewhat protective, with larger benefits for males than for females.4 We can’t extrapolate out to, say, the level of professional basketball players, but we can extrapolate out to every level that’s reasonable, and we can conclude that more height ultimately doesn’t look to be bad, and at the point where it might be bad, it’s only slightly so, and thus is likely ‘worth it’ from the child’s perspective.
But let’s add a final note here: the main source of risk from greater height is cancer, and we’re getting much better at treating cancer all the time. By the time children come to the rather advanced age where cancer is a real risk to them, we’ll likely have made significant progress, and possibly abolished some of the types of cancer they might face, leaving us with significantly greater upside.


Or, in other words, the case for making your kids taller is getting better all the time, and the case that you’re shortening their life by doing so keeps getting weaker.
