
I Don't Believe In 'Gluten Intolerance'
There's no convincing evidence for 'non-celiac gluten sensitivity'

This was a timed post. The way these work is that if it takes me more than an hour to complete the post, an applet that I made deletes everything I’ve written so far and I abandon the post. You can find my previous timed post here.
Grocery stores are filled with gluten-free bread, sweets, and pastas that look odd and taste worse. Not only that, there are also plenty of gluten-free replacement suggestions like swapping spaghetti with zucchini noodles, replacing tortilla wraps with lettuce, using cauliflower rice instead of cous cous, or putting a portobello mushroom on your beef patties instead of opting for a traditional hamburger bun.
A lot of this has to do with the rise of non-celiac gluten sensitivity (NCGS): supposed harms from the consumption of gluten among people who do not have the celiac autoimmune disorder that causes the body to bloat, become anemic and tired, and induce diarrhea when gluten is consumed. NCGS sufferers claim to have many of these same issues without having the genetic causes or the inflammation that marks traditional celiac disease.
Despite its impact on grocery stores, restaurants, and the memeplex, seeming to verify that it’s real and the market is responding to something substantial, NCGS has all the hallmarks of a disease that’s not real, at least in its own terms. I’ll clarify what I mean by example:
Do you know the difference between inflammatory bowel disease (IBD) and irritable bowel syndrome (IBS)? They have similar acronyms, and they both appear to be about the gut, but that’s about where the similarities end.
IBD is an umbrella term for autoimmune inflammatory conditions like Crohn’s disease and ulcerative colitis, whereas IBS is a ‘Disorder of Gut-Brain Interaction’, or DGBI. DGBIs don’t appear to come with any functional or structural gut problems, but instead arise from people with irritable minds disturbing their guts: they get stressed, they eat poorly, they get annoyed by minor issues that more resilient people might be able to brush off, and they imagine symptoms that probably aren’t there. It’s usually the case that IBS looks more like a mental disorder than a bona fide bowel condition. It is meaningfully psychosomatic.
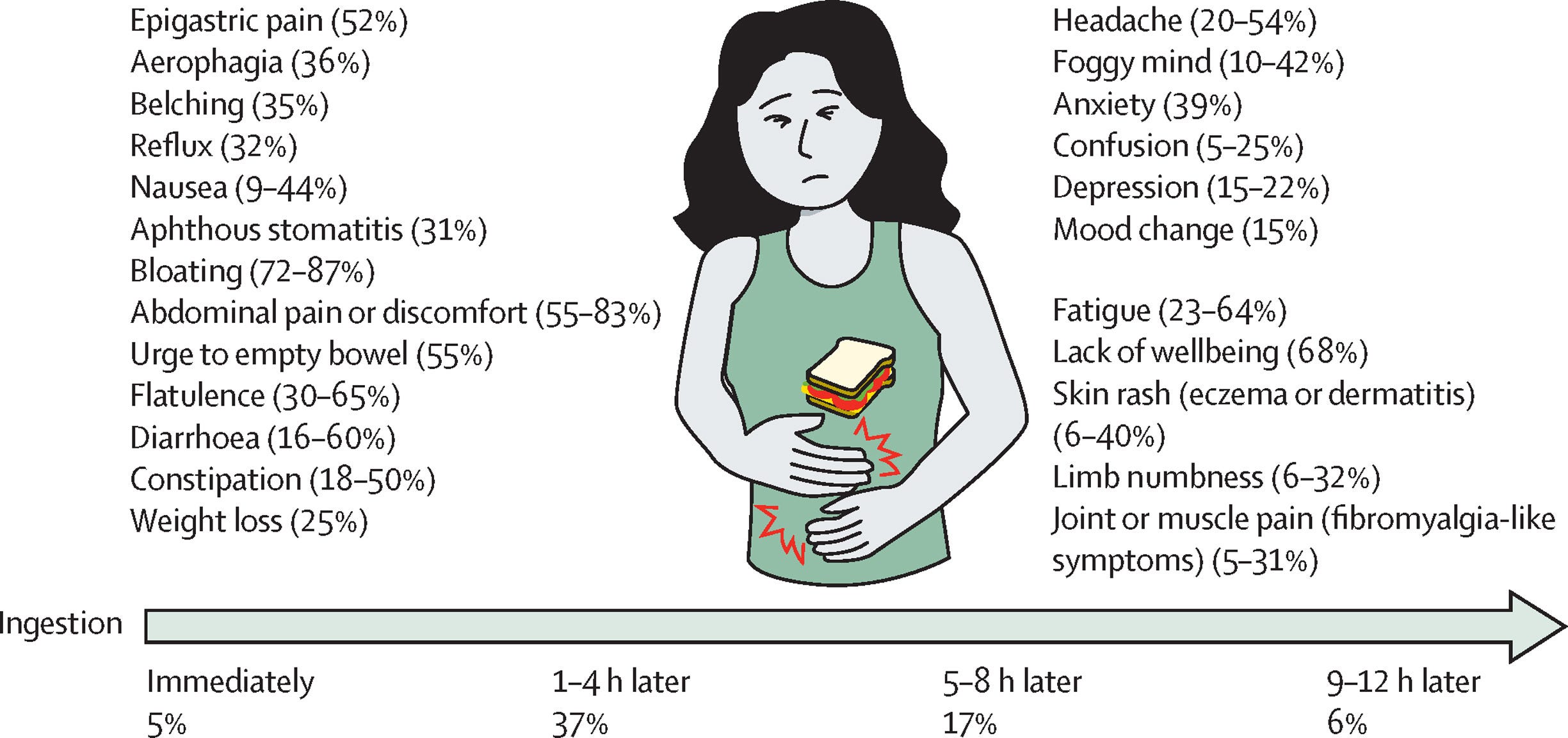
IBS and NCGS are overlapping conditions, whereas IBS and celiac disease have much less overlap. NCGS sufferers are also about 70-80% female, whereas celiac disease is much more evenly split by sex (~55-60% female). Celiac disease is largely gastric and presents with a variety of physical symptoms, whereas NCGS commonly presents with symptoms like headache, brain fog, anxiety, confusion, depression, fatigue, and diffuse pain—all of which are marked symptoms of other largely-psychosomatic illnesses like long COVID and fibromyalgia. Moreover, celiac diagnosis tends to be symptom-driven following a clinical work-up due to specific symptoms or an incidental finding during other evaluations, while NCGS diagnosis is usually a self-diagnosis or something suggested by an alternative medicine doctor or dietitian rather than a real doctor. And, while untreated celiac disease is associated with a wide array of nutritional deficiencies, the association between NCGS and nutritional deficiencies is both different and less extreme.
NCGS looks like a DGBI, not a genuine autoimmune disorder, and it is certainly not what it appears to be. NCGS is definitely not about reactivity to or an intolerance of gluten per se. The best way to grok this is to look at the results of the landmark challenge studies highlighted in last year’s Lancet review.
The seminal publication on NCGS is Cooper et al.’s challenge study from all the way back in 1980. In it, Cooper et al. subjected eight adult women without celiac to eating a diet with gluten and after they did, they saw some meager signatures of gastrointestinal response. Later reviews have flagged this as low-quality evidence for NCGS, but it’s worth mentioning because it’s the first real clinical report we have.
After the popularity of the condition had grown, we got another study some thirty years later. This was a double-blind, placebo-controlled (DBPC) trial including 34 non-celiac patients, where 68% of the patients given gluten-rich food reported inadequate NCGS symptom control, compared to 40% of those who were not given gluten. All of the effects, however, were subjective, and there was nothing to show for anti-gliadin antibodies, fecal lactoferrin, celiac antibodies, hsCRP, or measures of intestinal permeability.
Two years later, the same research group did another DBPC trial, this time taking aim at a possible connection between NCGS and IBS. In this trial, they gave their 37 non-celiac participants diets that were low in FODMAPs—the types of carbohydrates that make you feel gassy and bloated—and then placed them on high-gluten, low-gluten, or control diets. With low FODMAPs, participants were a lot better off, and when they were exposed to the higher FODMAP diets, they got worse, but not especially so with gluten.
This is key: people with DGBIs like IBS tend to be sensitive—hypersensitive, in fact. When they eat things that would make any of us bloated, they seem to feel much worse than we do. With the same bloating, the same gut distension, the same gassiness, they report feeling relatively excruciating pain, where normal people would feel practically nothing. A subset of them—one that’s more female and rates higher on several additional mental disorder measures—also frequently report feeling more pain broadly, and these individuals have less complete recovery when they’re put on a low FODMAP diet, because their issue is a broader pain perception one (or at least, that’s how they report it),1 and relieving painful bloating is only a partial fix.
A study the following year showed practically no reaction in a 22-person DBCP trial of non-celiac NCGS sufferers, with the only reaction being psychological (p = 0.01 for one of two possible dietary subgroup comparisons on a depression subscale score for the STPI) rather than physical (cortisol, gastrointestinal symptoms).
The next year, a 35-person DBCP trial assessed NCGS sufferers’ ability to distinguish gluten-containing from gluten-free flour. They found that surreptitiously exposing participants to gluten only elicited symptoms in one-third of NCGS patients, with just 34% even correctly identifying gluten flour and 49% incorrectly identifying a gluten-free flour as having gluten in it. Among those who incorrectly identified the gluten-free flour as containing gluten, they had stronger reactions. In the same year, a 61-person DBCP trial of non-celiac NCGS sufferers came out. In it, participants either took gluten or rice starch capsules, and the result was p-hacked: the authors registered that they would report on 15 intestinal symptoms and 13 extraintestinal symptoms, but they ended up only reporting the ones that showed significant differences, and each such difference had a p-value that was dubious, ranging from 0.019 to 0.047. And, only 3 of 59 subjects who completed the study showed any evidence of gluten sensitivity—consistent with chance!
In 2018, another DBCP trial found FODMAP (specifically the ‘O’, fructans) sensitivity rather than gluten sensitivity. That year, we also got a DBPC in children, with 1,114 gastrointestinally-dysfunctional children enrolled and the 3.3% who showed a correlation between gluten ingestion and symptoms taken off to do a crossover gluten diet challenge. Among those kids who did the challenge, 39% showed worse symptoms with gluten, but the majority showed no evidence of any issue, and the number of those who showed an issue is absolutely small. More pressingly, the p-values for group differences are misreported and a few challenge results that are reported as significant are instead nonsignificant and misreported. For example, in Table 3, results reported as p < 0.005 or <0.001 were instead 0.030, 0.082, 0.498, and 0.027.
Finally, we got a larger, stronger study of 84 NCGS sufferers. This one had a unique factorial design in which participants were sorted based on the expectation of eating or not eating gluten, and then they were also given or not given gluten within different expectancy groups. Expectancy—not actual gluten content—dominated. The participants who expected gluten and got it or did not get it had comparable responses, and those who didn’t expect it weren’t affected. Or, in other words, there was a nocebo effect: the anticipation of gluten was the source of the problem. Gluten was innocent! In other trials (and, indeed, in reviews), nocebo effects crushingly outnumber anything that could look like actual gluten sensitivity (but which might in truth be FODMAPs or some other stimulus).
The picture we get from challenge studies is one in which NCGS looks like little more than IBS, complete with the same demographics, similar treatments, and anticipation effects that show it’s substantially psychological in nature. Meanwhile, there’s no meaningful or consistent evidence for gluten actually being involved. Despite extensive searching, there are no NCGS biomarkers, nor any identifiable severe acute reactions, and there’s no evidence of physical effects on the gut, immune reactions, or anything you might expect if people are, as they think, sensitive to gluten.
There is no reason to believe that a non-celiac sensitivity to gluten actually exists.2
How Do We Treat Mental Illness Disguised as Food Issues?
But there are still NCGS sufferers, people who wrongly think that they’re affected by gluten when they’re suffering due to something else. These are people who are more likely to have IBS or some other functional gastrointestinal/mental disorder characterized by hypersensitivity and typically alleviated through dietary restrictions intended to cut down on or distract them from specific, generally tolerable conditions like bloating and gas. They usually have mental comorbidities and they frequently claim to have a bundle of other conditions that are not what they seem.
The easy answer on what we should do for these people is to restrict their diets in a way that alleviates their symptoms by cutting out FODMAPs, fructans, or whatever else contributes something towards states they’re hypersensitive to. To the extent—which is major—that their symptoms are ultimately due to some sort of mental illness, we’ll need to keep looking at that angle. It would be unethical to only treat what might be a delusion built from a mental illness when it could be possible to treat the underlying mental illness that creates false food sensitivities.3
Their pain reports have a clear psychological element, as evidenced by antidepressant and antipsychotic trials, which shouldn’t do anything to pain—and, indeed, these drugs do not function as painkillers normally—nevertheless helping to reduce rates of broad pain-related symptom reports.
And wheat allergies are different, not usually supported in actual allergy testing when they’re based on self-reports, and they’re not about gluten.
This applies to many things like NCGS, too. These range from nonexistent allergies to supposedly—but not actually—trauma-driven pain to mold-caused respiratory and cardiac symptoms without any actual mold involvement.
Interesting, thanks! I suspected this but it would be impolite to challenge a friend about. (All female)
FODMAPs is an interesting angle. Maybe those tend to have gluten and it results in an incorrect assignment of blame?
I do wonder how gluten took such a spotlight to be mentioned everywhere.
My wife has celiac disease and we have long suspected that most of the people purporting to need to avoid gluten are kind of hypochondriacal. Still, I feel kind of ambivalent about their behavior. On the one hand, it has helped make "gluten-free" the butt of innumerable jokes (to the point that now mocking gluten-free demands is kind of passe/cringe), and makes people who just meet us probably a little more suspicious that she is BSing and therefore annoying to accommodate.
On the other hand, the consumer demand from all these fakers and hypochondriacs has indisputably helped power the great ingenious engines of capitalism to invent, import, and serve much more abundant selections of gluten-free substitutes, as well as to nudge things that were by default nearly gluten-free the rest of the way. Like gluten-free cheerios! This change has been remarkable, from when we started dating in 2010. Although the main adaptation we used back then remains really fun: just starting with cuisines that don't rely on gluten in their staple grains, like Mexican, Thai, Vietnamese and Japanese (subbing Tamari for soy sauce).
At the end of the day, she cares far less what some rando thinks of her maybe faking it, and far more about the availability of things she can eat.