
Is It Possible to Be Healthy at Every Size?
Just what is "metabolically healthy obesity" and should we care?

This was a timed post. The way these work is that if it takes me more than an hour to complete the post, an applet that I made deletes everything I’ve written so far and I abandon the post. You can find my previous timed post here. I placed the citation list at the end before I began writing the rest of this.
Have you ever heard about “HAES”? It stands for “Healthy at Every Size” and it’s the idea that people can be healthy regardless of how fat they might be.1 This idea might sound surprising given what we know about how obesity affects health.2 And yet, it has garnered a degree of intellectual cachet. In fact, it’s inspired some meaningful empirical research into the condition of being both fat and healthy, a condition known as metabolically healthy obesity, or MHO.
MHO is a poorly-defined idea.
A review of the MHO concept by the nutritionists Smith, Mittendorfer and Klein (SMK) noted that there “is no universally accepted standard for defining MHO, and more than 30 different definitions have been used in different studies”. Most studies define MHO based on being obese while having some small number of the symptoms of metabolic syndrome.3 That sounds fair enough: MHO is basically defined as having some signals of looking healthy and being obese. But is this even necessary? How prevalent is MHO versus its antithesis, metabolically unhealthy obesity, MUO? In the CDC’s nationally-representative NHANES dataset, the answer is ‘fairly uncommon.’
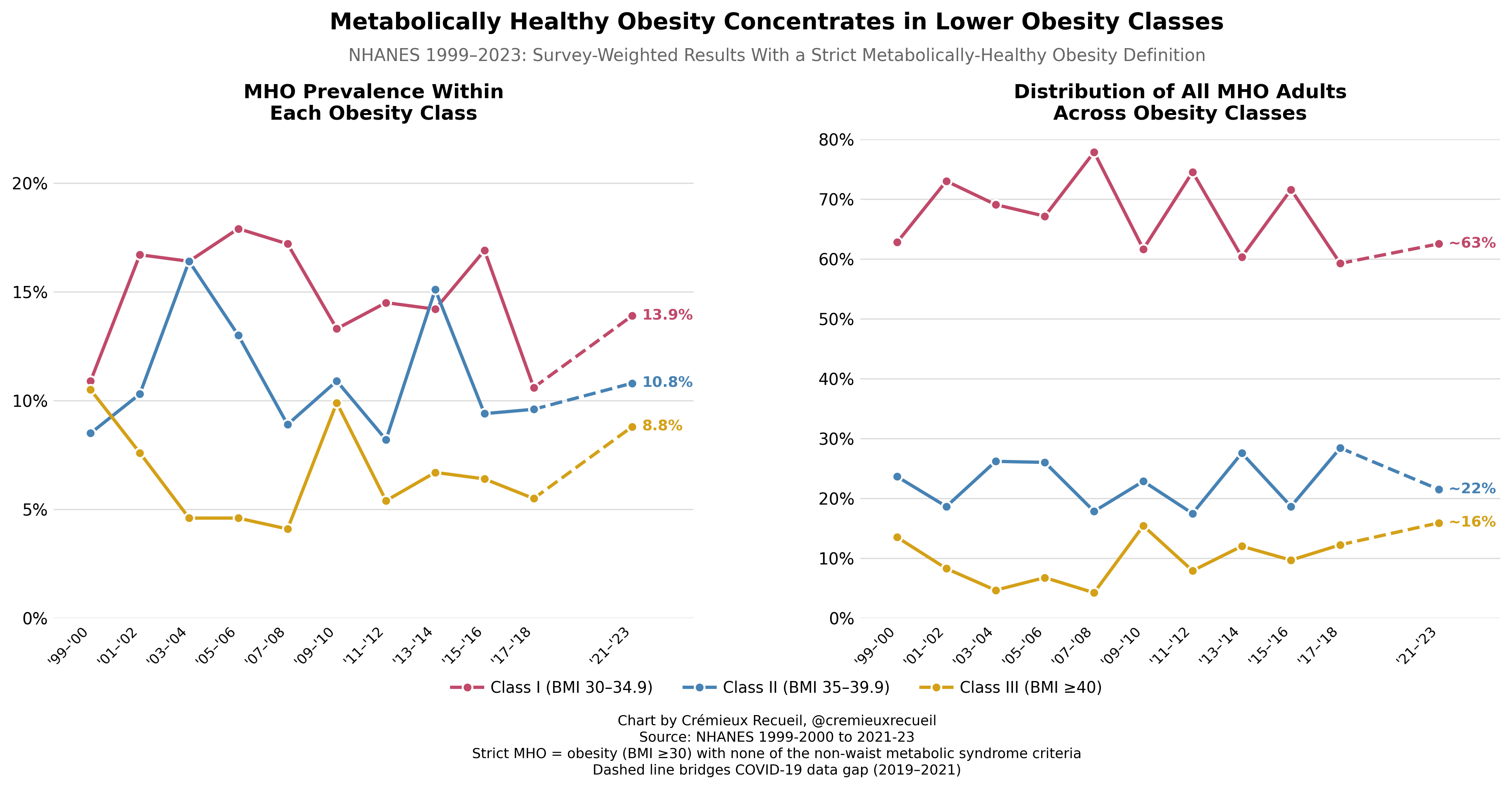
8.8 to 13.9% of each obesity category qualified as MHO in the latest sampling year based on a fairly strict definition I found had been used in this dataset by Wang et al. Because more of the obese are Class I (i.e., BMIs of 30-34.9) than are in the higher BMI classes, the majority (about two-thirds) of those who are MHO are borderline obese, and with more extreme obesity, MHO is rarer relative to MUO. This is consistent with the findings of the SMK review:
In general, MHO is more common in women than in men, in younger than in older adults, in people with BMIs less than 35 kg/m2 than in people with BMIs of 35 kg/m2 or higher, and in people of European ancestry than in those from Africa, South America, and South Asia (Indian ancestry).
Notice the line “MHO is more common… in younger than in older adults”. This is crucial. MHO is unlikely to be a stable condition. I tried to find every study that examined how people converted between MHO and MUO and found a lot of them, and they generally agreed: the more time that passes, the fewer people maintain MHO.
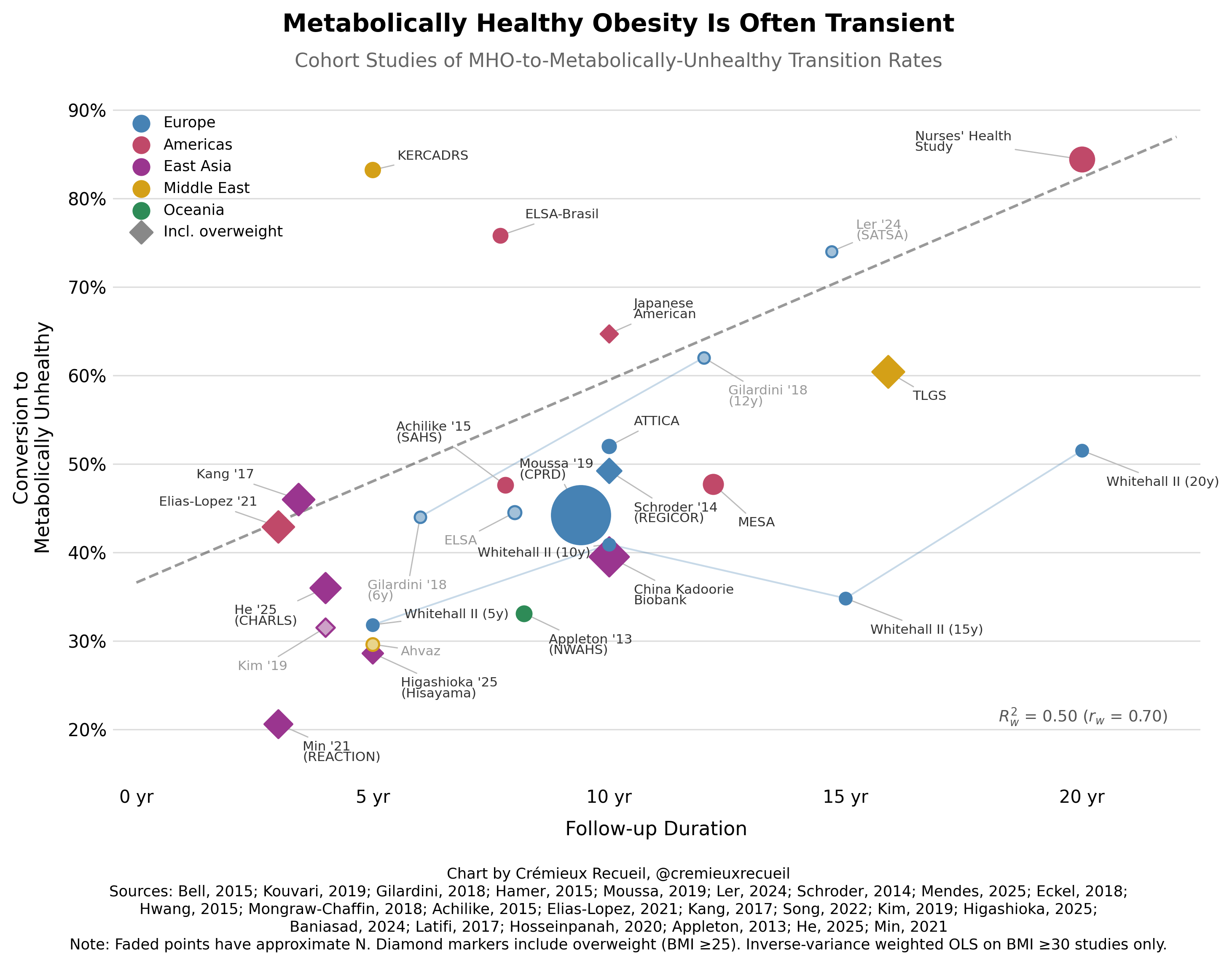
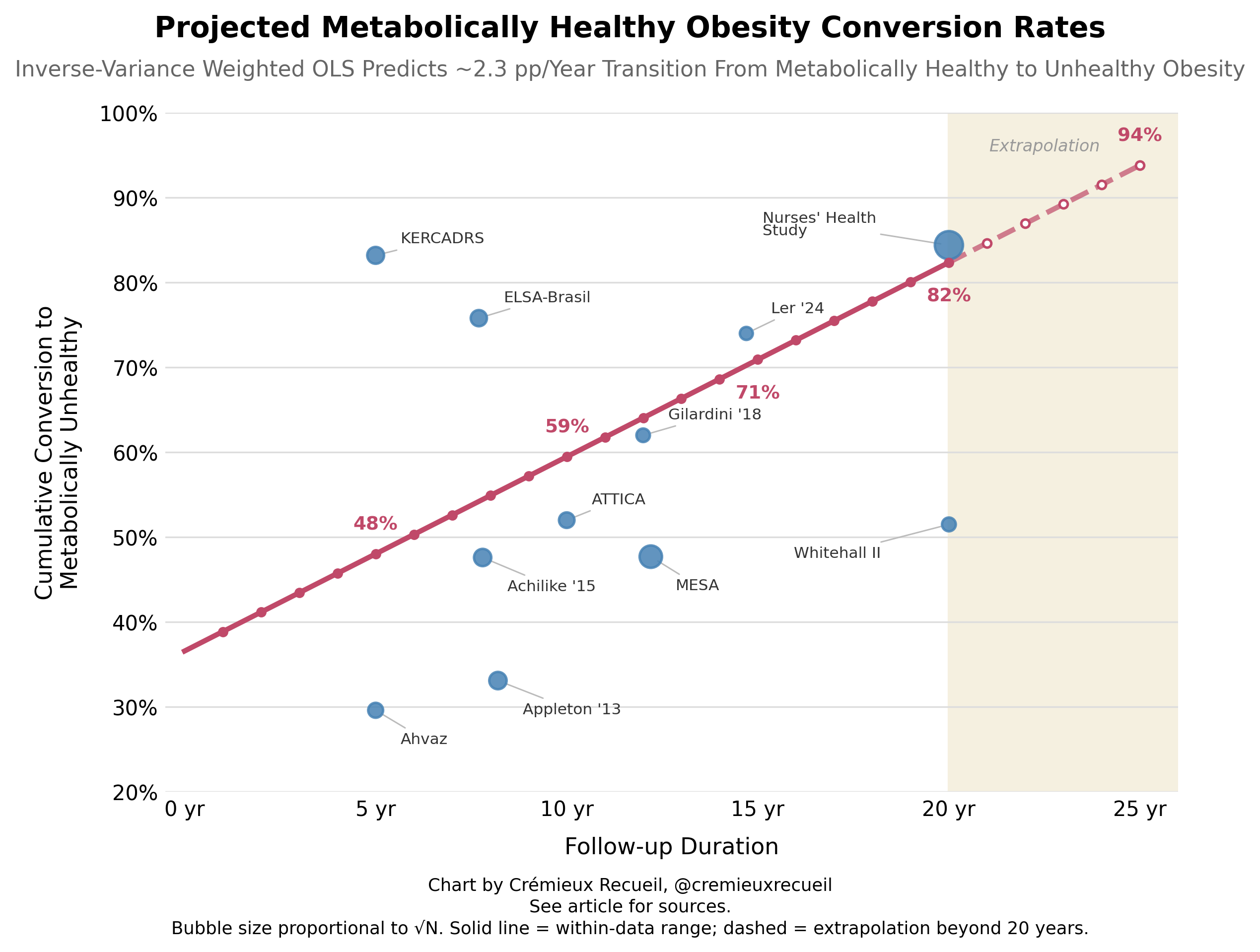
Though I’m not confident in the appropriateness of this analysis, it is possible to take the results from these different studies, with all their differences in definition noted, and to make a projection about how stable MHO can be. If we do that, it looks like 8-9/10 cases of MHO become MUO by 20 years in. That’s a theoretically dubious estimate, but I imagine something like it is not that far off the mark. Majority conversion in that time is highly believable.
MHO is defined as obesity with a reduced but not zero metabolic downsides typically associated with obesity, and… it’s not very protective.4 A few select quotes from SMK should suffice:
The risk of developing T2D is much lower in those with MHO than MUO, but is still about 4-fold greater than in those who are MHL [i.e., metabolically healthy and lean], and is directly related to the number of metabolic abnormalities at baseline….
The risk of CVD events (new-onset angina, fatal and nonfatal myocardial infarction, sudden cardiac death, fatal and nonfatal heart failure, and peripheral vascular disease) is lower in people with MHO than in those with MUO, but is still higher in people with MHO than in those who are MHL….
The combined data from five large cohort studies that followed participants for an average of 13 years found that people with MHO and no metabolic syndrome components (excluding waist circumference) did not have an increased risk of all-cause mortality compared with the MHL group; however, the risk of all-cause mortality was greater in participants with MHO versus MHL when participants with one abnormal metabolic risk factor (excluding waist circumference) were included in the MHO group.
The people who are MHO are still at a high risk, and because so many of them convert to MUO, the risk is higher than it might appear at a given ‘healthy’ baseline because so few can stay ‘healthy’. And this has a lot to do with fat itself being bad and, like cholesterol, causing damage that accumulates over time.5 We can see this in a variety of ways.
For one, we know that being fat is bad for glycemic parameters—that is, blood sugar. Bad glycemic parameters lead to cumulative damage because they’re constant stressors on numerous areas of the body, and perhaps also because they lead to obesity. In long-term follow-ups, there’s evidence of metabolic memory such that earlier periods of better or worse glycemic control affect complication risks years down the line. Patients that engage in early, intensive glucose control efforts also show reduced rates of microvascular complications, with numerous systemic benefits including, notably, reduced risk of all-cause mortality.
Mendelian Randomization supports the idea that BMI and abdominal adiposity are causally linked to both insulin resistance and type-2 diabetes, but not clearly to fasting glucose itself. This fits with obesity mostly wrecking insulin sensitivity first, with fasting glucose remaining compensated for a while. An individual could appear ‘MHO’ while being on a path to MUO as their insulin sensitivity degrades.
Moreover, one of the things that predicts going from MHO to MUO is visceral fat accumulation—which tends to happen with time spent being MHO and MUO alike—, and visceral fat seems to be itself bad for glycemic parameters. As a sort of natural experiment, people with lipodystrophy also tend to develop severe insulin resistance, hypertriglyceridemia, fatty liver, and diabetes. However, it’s not clear that just removing this fat fixes the issue. Liposuction cases don’t seem to show improvements in insulin action and glycemic control.
For two, obesity is harmful through mechanical load. Having more tissue also predicts, and quite likely causes, higher rates of cancer, in addition to all the other carcinogenic effects of obesity. It directly leads to sleep apnea and hypoventilation; fatty liver and liver fibrosis; osteoarthritis and musculoskeletal damage; venous thrombosis and impaired fibrinolysis; kidney damage; adverse adipokine signaling; chronic low-grade inflammation; and by being fat, you’ll probably be respected less, leading to whatever health harms follow from being socially rejected and disliked more than might be the case if you were skinnier.
If you’re a guy, you should be worried by obesity because it lowers total and free testosterone and raises the estrogen to testosterone balance because adipose tissue expresses aromatase, which converts androgens to estrogens. As a result, obesity can lead to gynecomastia, lower libido, erection problems, worsened fertility, and reduced muscle mass—obesity-related sarcopenia! For women, the worry runs the opposite direction, with obesity being relatively masculinizing, contributing to the worsening of PCOS and hyperandrogenic abnormalities that can impair fertility.
I could go on.
My point is this: Healthy at every size is quasi-mythical. There are people who appear to have relatively normal metabolic parameters while being obese, but they are generally not very obese, just somewhat fat. Moreover, few of the seemingly healthy obese people can sustain whatever metabolic healthfulness they have for very long, and to the extent they can, it’s probably because whatever damage they’re accumulating isn’t being measured or isn’t being used to define that person as metabolically unhealthy even though they’ll soon become metabolically unhealthy by any measure.
If we want people to be as healthy as possible, we’ll not humor the idea that people can be healthy at every size, because, frankly, it’s just not true.

The studies referenced in the charts are ATTICA, ELSA-Brasil, the Nurses’ Health Study, Hwang et al. (2015), Kang et al. (2017), MESA, KERCADRS, the Kadoorie Biobank, Ahvaz, Gilardini et al. (2018), ELSA-England, Kim et al. (2019), TLGS, NWAHS, CPRD, REGICOR, Whitehall II, Achilike et al. (2015), SATSA, Elías-López et al. (2021), Higashioka et al. (2025), CHARLS, and REACTION.
Specifically, it is a weight-neutral, non-diet approach to health that emphasizes supporting healthy behaviors rather than pursuing weight loss. But the idea behind it is that you can be healthy by doing those things, even if you are fat. Hence how I’ve defined it there.

In the papers linked at the end of this article, I noticed that the definition used in analyses of the NHANES, ATTICA, and ELSA-Brasil cohorts were stricter than the definitions used in the Whitehall II, ELSA-England, and REGICOR cohorts, which themselves had stricter definitions than the MESA, TLGS, China Kadoorie Biobank, REACTION, and CHARLS studies used. The studies with the least comparable definitions to the NHANES one relied on diagnoses and administrative coding; those were the Nurses’ Health Study and CPRD.
It’s also not very productive to aim for MHO, as there are no consistent dietary or behavioral predictors of it, and people seem to convert to MUO regardless of those things, if you give them a long enough window of time. Moreover, several of the characteristics of MHO appear outside of the control of the individual. These include factors like visceral fat, lp(a) levels, rates of lipogenesis, adipocyte size, oxygenation, adiponectin levels, etc.
Some people will object that some of the MHO are likely to be bodybuilders who are classified as obese while being highly muscular. For one, bodybuilders are often metabolically unhealthy, with bad cholesterol levels and the downsides associated with steroid use, which can be extremely severe. Such states are usually unsustainable, too. For two, BMI and actual adiposity measurements rarely disagree, so if bodybuilders are included in MHO, they are not swaying things very much in any case.


Now that remaining obese has become effectively optional thanks to GLP-1RAs, I think it's fair to compare the the language and claims about MHO to other behavior with extremely strong causal correlations with bad health outcomes.
Can you find "cardiovascularly healthy smokers"? Probably, sort of, if you look hard enough. I'm sure cigarette apologists at least had no shortage of examples of smokers who never got emphysema or lung cancer. And alcohol apologists could point to regular drinkers who happened to maintain liver and kidney function. But like with MHO people, it is very telling that such individual exceptions got rarer at older ages / longer durations of regular smoking and drinking. Some persisted into old age! Good for them! But in no other area of medicine would we say "the existence of some exceptions to the rule in a population of millions means that the rule is false and shouldn't be used to advise changes in behavior."
To be fair, you’d need to control for IQ for observational studies that look at the downside of obesity. There was one Swedish study that did this (via education) and found that high obesity was associated with bad health, but the BMI-health curve was shifted by education (higher educated are healthier at every level of BMI and vice versa).