
Did The HHS Just Explain Autism?
One-word answer: "No." But it is going to hurt a lot of mothers and autistic people.

The Department of Health and Human Services (HHS) and its subagencies have been hard at work since inauguration. They’ve been trying to overcome the daunting task of figuring out: Why’s there so much autism? After eight months, they finally gave the press conference revealing what they learned, and all of it was wrong. They alleged:
Acetaminophen (Tylenol/Paracetamol) use during pregnancy causes autism
Folic acid deficiency causes autism
Those were their key claims and the basis for their advice to tell mothers to avoid Tylenol while pregnant and for Centers for Medicare & Medicaid Services (CMS) to start covering the drug Leucovorin. In addition to these claims, they also had several other erroneous claims and inferences, such as:
The Amish don’t have autism
Diagnostic drift isn’t an explanation for the autism “epidemic” because:
California’s M.I.N.D. Institute debunked diagnostic drift
There aren’t many old people with severe, head-banging-against-wall autism
We aren’t listening to mothers of kids with autism, who are sure that their autistic children resulted from vaccine injuries
MMR vaccination causes autism and it would be safer and result in a lower total dosage of vaccine if it’s split up
Cuba doesn’t use Tylenol and they have low autism rates
The HHS left no stone unturned in reaching these conclusions
Let’s briefly go one-by-one and eventually describe three things:
How things came to this
What will now happen to mothers and people with autism
What should have happened//How Trump can get a layup
Before getting to that, I’m going to recommend that you go read my post on the causes of the autism epidemic. It’s not long, and it covers all the bases:
What’s the Deal With Autism Rates?

One of the major priorities of the new Secretary of Health and Human Services (HHS), Robert F. Kennedy Jr. (RFK Jr.), is to figure out why rates of autism have been increasing over time.
Does Tylenol Cause Autism?
The answer here is “no”. We know this because of an incredibly strong research design applied to an incredibly large sample: a sibling control study applied to a population register including nearly 2.5 million births.
A sibling control study is a simple, informative design. It entails comparing someone who was exposed to one thing—in this case, Tylenol in utero—and comparing them to a sibling who was not exposed to that thing. The researchers who looked into this had access to data on multiple births from different methods between 1995 and 2019, followed up through the end of 2021. They measured Tylenol usage during pregnancy based on two methods:
Midwife reports from structured interviews of mothers, coupled with physician reports
The centralized, Prescribed Drug Register, which records all drugs given out in the country after July 1, 2005
Results using both exposure measures agreed: there is no causal link between Tylenol use during pregnancy and autism. Why? Because the exposed sibling was no more likely than the non-exposed sibling to actually go and develop autism or, for that matter, ADHD or mental retardation (intellectual disability). The result is incredibly clear: there is a correlation between Tylenol usage across mothers, and higher doses are associated with greater risk of the condition, but there is no association between siblings, so the correlation is due to familial confounding. Study the chart:

The study also found, between siblings, associations with aspirin, opioids, anti-migraine drugs, and non-aspirin NSAIDs were fully attenuated. To repeat: they were fully attributable to confounding!
So, in light of this, why did the HHS say that Tylenol causes autism? Because of an incredibly irresponsible review by an incredibly irresponsible researcher with an incredibly irrelevant background and an incredible lack of self-awareness about the limitations of his methodological know-how. Here’s a link to the review in question.
The authors did, indeed, cite this sibling study. But they dismissed it in favor of non-causal evidence. Why? The most likely reason has to do with the credentials of the authors. The lead author is the Dean of the Harvard School of Public Health; moreover, he’s appeared as an expert witness in court on this very topic. But his expertise is, evidently, quite limited. Take his review as evidence. Instead of accepting the strong, causal evidence provided by the sibling control studies in this literature, he instead lied about them:
exposure assessment in this study relied on midwives who conducted structured interviews recording the use of all medications, with no specific inquiry about acetaminophen use.
We know this to be false. Exposure assessment was done by midwives and physicians, but it was also done through the Prescribed Drug Register where all drug prescriptions are recorded, and the result was the same. So that’s a lie! He goes on:
Possibly as a resunt [sic] of this approach, the study reports only a 7.5% usage of acetaminophen among pregnant individuals, in stark contrast to the ≈50% reported globally.
But this is also in error! The authors of the sibling control study explicitly documented that their exposure numbers were typical. For example, they noted high pre-pregnancy usage among eventual mothers in neighboring Denmark, which collapsed to levels like what they observed by the first trimester. He then states:
Indeed, three other Swedish studies using biomarkers and maternal report from the same time period, reported much higher usage rates (63.2%, 59.2%, 56.4%)
Curiously, the review only cites one of these studies after that statement, the source of the middle estimate of 59.2%. The 59.2% estimate is self-reported from a select cohort of women enrolled in pregnancy weeks 8-13, and the number refers to usage between conception and enrollment, not just during pregnancy. But, as noted in the sibling study Baccarelli handwaved away, women’s use of Tylenol declines going into pregnancy, so the period the survey refers to needs to be understood in this light.
Baccarelli clearly miscited this study as if it was more relevant than it is. As an aside, the study found that self-reported use at any eligible point was associated with urinary levels at enrollment (r = 0.29) and there was no overall association between usage of Tylenol and learning disabilities in this study. The authors did try to go on a fishing expedition, but they wound up with some marginally significant effects without supportive interactions. Baccarelli continues:
Additionally, while sibling comparison studies eliminate the impact of shared family factors that operate as confounders, they also eliminate potential mediators that are shared in families that interact with acetaminophen, potentially introducing bias.
Baccarelli should have realized that a causal theory still implies that the sibling estimate should be dragged towards the population estimate. Baccarelli apparently did not appreciate this, so he left this in not knowing that it’s just evidence of him throwing anything he can against the wall in the hopes something sticks. Moreover, it’s very clearly just an inconsistently applied excuse, since he failed to offer any plausible mediator candidates (and indeed, there are none; I looked through the genetic evidence here, and that offers no support). A mediator must lie on a path from that sibling’s exposure to that sibling’s outcome (E → M → Y). A variable that is truly shared (i.e., constant within the family) cannot be changed by one sibling’s pregnancy-specific exposure, so it can’t mediate the between-sibling effect.1
The bias to watch out for in sibling control studies is one where acetaminophen usage in pregnancy for Child-I changes a family-level state that persists and affects Child-II. That’s “carryover bias” or “interference” and it’s a SUTVA violation. In that unusual case, within-family estimates can be biased, but the problem isn’t “eliminat[ing] mediators” but instead, exposure-induced changes to shared factors across pregnancies. The actual weaknesses to worry about are non-shared, time-varying confounding (e.g., fever, infection, maternal age), measurement error (which is worse under fixed effects), and selection (only families discordant for exposures contribute to the sample). Unfortunately for him, none of these is a problem for the study he attacked.
Baccarelli continues:
A recent simulation study demonstrated that both controlling for mediators and underreporting acetaminophen usage could severely bias neurodevelopmental associations toward the null, reducing the observed effect.
At this point Baccarelli was taking issue with two non-issues, but it’s important to note: the study he cited here didn’t even understand the sibling study cited above. The study argues that “the vast majority of the raw (unadjusted for any potential confounding factor) risk was eliminated by adjustment for more than 20 inflammation-related or associated factors. That is to say, the vast majority of the risk was eliminated by adjusting for inflammation-associated factors in the analysis, not by adjustment for the sibling pairs.” But this is both (1) not true—go read the model specification from the sibling study!—and (2) really not true, because balanced factors were not controlled for within sibling pairs. What would it even mean to control for them? And furthermore, why not just ask for the crude sibling-controlled results?
We know what Baccarelli was doing! He was just throwing out whatever reasons he could think of to dismiss evidence he didn’t like, because he really wants the link between Tylenol and neurodevelopmental risk to be real, presumably so he can say that in courtrooms. There is quite literally nothing to the argument that Tylenol is linked with autism or any other neurodevelopmental disorder beyond shoddy cross-sectional research and absurd mechanistic studies (and we know mechanistic studies do not substitute for real statistical evidence; Baccarelli’s preferred studies—largely based on biased recall—do not either). The citations otherwise fall short in light of the strong causal evidence available to us, and Dean Baccarelli should be sanctioned for his inappropriate remarks, including his lying.2
Does Folic Acid Deficiency Cause Autism?
If you want to get better informed on this topic, go read my colleague Kevin’s article on this subject:

I’ll keep this section brief, and in it just relate two additional findings.3
Firstly, we have a society-wide experiment in whether folic acid is behind the rise in autism because at some point, we decided it was good to fortify food with folic acid. The result? A reduction in neural tube defects:

But, secondly, this had no effect on rates of autism diagnosis:
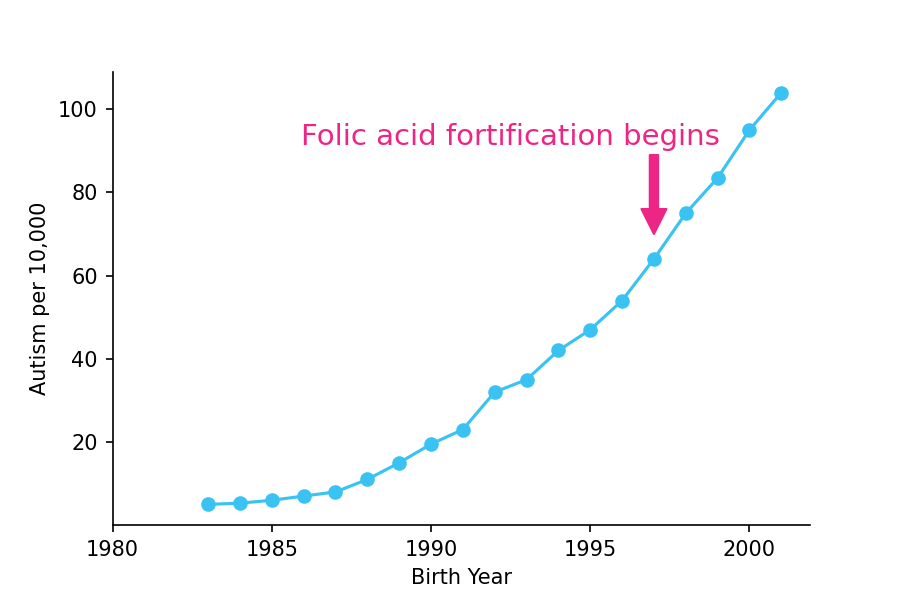
Folic acid fortification helped with conditions that were genuinely driven by a lack of folate, but it did not help with conditions like autism which were not driven by a lack of folate. That makes total sense, and it suggests that today’s move to cover Leucovorin will not be curing very many autism cases. It might help some kids with their symptoms, but the literature on this topic is weak, that I’m doubtful there will be measurable benefits at the population level. There will, certainly, be measurable harms though: tons of kids are going to take medication that’s not going to help them, and the taxpayer is going to pay for it!
Addressing Typically Unremarkable Tidbits
The Amish. For starters, the Amish shun technology, but many still vaccinate their kids. When researchers go out and check if the Amish have autism, they do find a non-zero rate of autism. The idea that they don’t have autism, much less that they don’t have autism due to being unvaccinated, is empirically wrong. I have previously addressed it, but here I’ll add something: a lot of autism diagnosis happens as a result of parent referrals and questionnaire responses. The Amish respond differently to questionnaires, so, as with international comparisons, you have to understand that numbers from distinct populations are not inherently comparable.
Against Diagnostic Drift. RFK Jr. cited two arguments against a reporter who asked about the issue of diagnostic drift. His first argument was based on a study that I’ve thoroughly debunked here. The conclusion of that study was that, if you can take children born in 1983-85 who were diagnosed with the DSM-III, and re-diagnose them with the less restrictive DSM-IV ten years later and they’re still autistic, then the “observed increase in autism cases cannot be explained by a loosening in the criteria used to make the diagnosis.” If you don’t understand why this is balderdash, then please, click that link for a further explanation of this obvious nonsense.
His second argument was based on another argument that I’ve thoroughly debunked here. The argument comes in a few forms. In one form, it’s that when he was a kid, he noticed fewer kids with severe autism. This makes sense because back when he was a child—and he should know this given his family and the fact that he visited family members in asylums—they were generally kept locked up in asylums. The other form of this argument is that there are definitely more of these kids today. The basis of this is conflating numbers about a category whose meaning has drifted (severe autism) with a personal perception. But the reality is that severe autism cases are up due to increased survival of severely autistic children, diagnostic substitution, the ability to diagnose people with autism and other disorders, and so on. There is no part that can be attributed to a real increase over time, and if there is some small part that is, it’s more likely due to advancing parental (paternal and maternal) age and potentially assortative mating.
Believe Women? At one point RFK Jr. said that people say the slogan ‘believe women’ but they don’t act on it in the case of mothers whose kids have been diagnosed with autism, who swear that their kids were vaccine-injured. That’s a good thing, because people’s biased personal recollections and submission of potential post hoc ergo propter hoc evidence should not be considered to be of the caliber of real scientific evidence. We should not believe all women when it comes to these sorts of claims, especially since we know they’re false. I have three remarks on this.
Firstly, meta-analytically, cohort studies do not even support associations between any type of vaccination and autism.

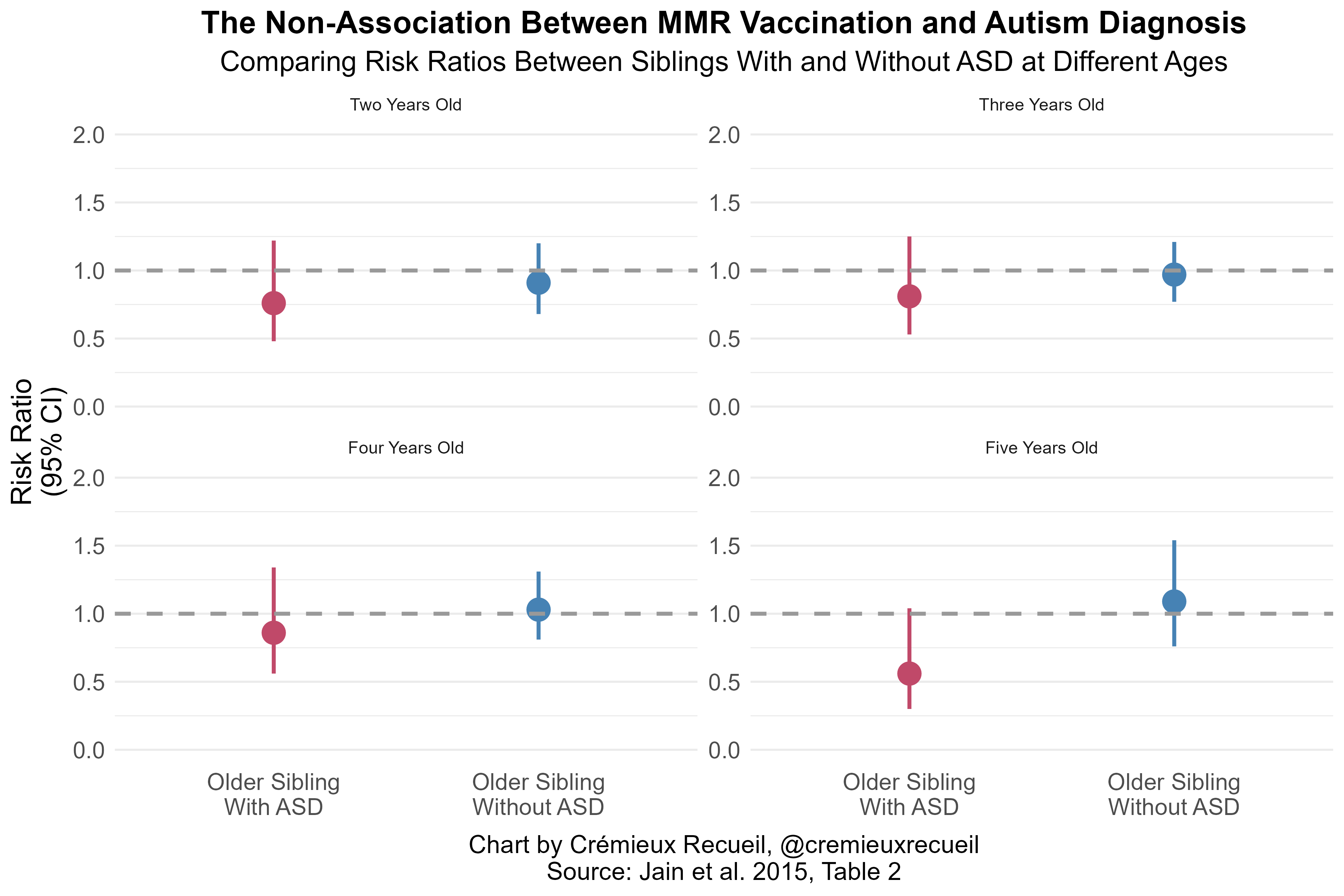
Secondly, MMR vaccination is not related to autism at any age when comparing siblings.
And finally, people need to get out of their heads. The only reason these mothers believe that vaccines made their children autistic is because they’ve been told it.
This is a frequent occurrence. A high-profile example has to do with talc powder (which the FDA is making moves against now, and which RFK Jr.’s son’s law firm is suing J&J over). Before the high-profile lawsuits against talc manufacturers, there was no case-control association between it and ovarian cancer; once it got in the media, people with ovarian cancer started remembering that they used talc powder. This sort of biased recall is the basis for the claim that talc causes ovarian cancer. If the idea wasn’t popularized, we would see what we see in cohort studies: namely, nothing!4

Split the Doses? Trump suggested splitting up the MMR vaccine after learning that ACIP recently split up the MMRV vaccine into MMR + V as separate vaccines. Why? Because he thinks it would help. He remarked that splitting these up would somehow reduce total vaccine amounts, but that’s obviously untrue. He just seemed confused on this. But we know the MMR vaccine is safe (see above), so he really just shouldn’t have made these remarks. He definitely should not have because, as a general rule, more difficulty means lower compliance. When you force parents to go to multiple visits to get their vaccinations instead of a single visit, you will inevitably have lower vaccine uptake.
This sort of thinking is why measles will be making a comeback.
Cuban Solutions? Trump said that he heard a rumor that Cuba (1) does not use Tylenol, since they can’t afford it, and (2) they have low autism rates. For one, Cuba does have both Tylenol and autism. Their rates are low, but you have to keep in mind that, firstly, Cuba is poor and awareness is low. Autism diagnosis is much more expensive than prescribing Tylenol, and the care that follows is even more so.
For two, as a general rule, you cannot compare numbers internationally. This applies to tons of things, from wealth on down to infant mortality. You have to do a lot to make numbers internationally comparable. Cuba is a good example of this because they completely fudge their infant mortality numbers. Poor countries frequently do things like this; for example, the Congo’s GDP numbers are just made up. But even in the U.S. over time, you cannot compare numbers. An example of this is maternal mortality, where the addition and roll-out of the checkbox drove an apparent—but not real—increase in mortality rates.
No Stones Left Unturned? I’m going to keep this very brief and a bit cryptic. I know the HHS received more causally informative data. I know multiple people at the HHS saw that data and some were even talked through it. It didn’t get any mention, but it completely debunks the claims made today and shows very clearly that diagnostic drift is fully explanatory for the rise in all types of autism.
While this stone might have been turned, it wasn’t acknowledged, and that’s just as bad.
How Did We Get Here? Where Can Trump Go?
How? This report emerged from erroneous beliefs promoted largely online by crackpots like David Geier, who produce non-science they parade about as public health informing, like this. Geier, it turns out, was appointed by RFK Jr. to help with the report that led to today’s press conference and its recommendations. He was presumably supported because he agrees with conclusions people already wanted to hear, and he’s perceived as an ‘outsider’—with good reason, it turns out. Appointing crackpots led to these unwarranted conclusions that will hurt a lot of people.
What Now? People do follow the advice of health authorities. Doctors often have to follow said advice, medical labels are updated to include warnings no matter how absurd, and our public health authorities exact a tremendous price on those who receive the wrong advice. So, two things: many mothers will now suffer through pain they could’ve reduced by taking Tylenol because they’re afraid and many mothers will substitute to Ibuprofen even though it isn’t safe, just because they don’t know any better. Secondly, a lot of kids will be given folic acid supplements for no good reason, resulting in a lot of waste paid for by taxpayers via CMS.
What Should Have Happened? Trump should have ended the autism epidemic. He easily could’ve. It would’ve been the easiest layup in history, and fully within his power, because he is the president.
Trump could have instructed RFK Jr. to follow the regulatory guidance I laid out here:
How To End The Autism Epidemic

This was a timed post. The way these work is that if it takes me more than one hour to complete the post, an applet that I made deletes everything I’ve written so far and I abandon the post. You can find my previous timed post here.
Had he done that, we would see an immediate reduction in the number of new diagnoses and a shift away from getting diagnosed with autism versus other, potentially more appropriate, diagnostic categories. Why? Because the autism “epidemic” is about incentives and diagnostic changes, and the president has the power to change those incentives and hem in those diagnostic criteria. The power is his, and he can still do it. If he wants to save the country billions each year and trillions in the near future, he will. But if wants unnecessary harm to befall pregnant mothers and autistic people, then he’ll instead continue with the actions suggested today, and we’ll all be worse off for it.
After writing this, someone asked me What if the mother’s genetics are driving things? To that, I’d note that existing GWAS results can already be used to cover this, and more importantly, that monozygotic twin concordance tends to be roughly twice the concordance for same-sex dizygotic twins. Given the lack of chorion effects—which you can infer from direct investigation or from similar dizygotic twin and full-sibling pair resemblance—, there’s really no way to explain this via the mother, and this is crucial to explain given the extremely high heritability of autism.
As an added note here, RFK Jr. mentioned the hepatoxicity of Tylenol as a knock against the product. Tylenol is very hepatoxic if taken in large doses, like the doses so many people end up taking: “Acetaminophen toxicity is the second most common cause of liver transplantation worldwide and the most common cause of liver failure in the United States.” Our best estimates suggest that half of these overdoses are unintentional.
RFK Jr. should fix this issue, because he can, and because it would be a good thing for public health. All he has to do to ensure zero people overdose from Tylenol is to update the monograph for the drug so that manufacturers can bundle it with N-acetylcysteine. This drug “is almost 100% effective [for acetaminophen toxicity] if given within 8 hours post-ingestion” and it doesn’t impair the therapeutic benefits of taking Tylenol. It fully eliminates Tylenol’s toxicity if administered alongside it and it is itself safe to take. Many bodybuilders use it as a supplement for liver health. So, to prevent any more deaths from the hepatoxicity of Tylenol, simply update the monograph so manufacturers can sell ‘liver-safe Tylenol’.
Another argument, which I don’t see any need to address, is that cerebral folate deficiency (CFD) is extremely common among ASD sufferers, so leucovorin is likely going to help if massively prescribed to people with ASD. For one, CFD should’ve still been reduced by fortification, but nothing changed. For two, I don’t believe the rate is as exorbitantly high as people like to suggest.
The most common estimate I keep seeing comes from this study. It apparently finds a 44% ASD prevalence among people with CFD and a 38% CFD prevalence among people with ASD. These numbers are insanely unrealistic and it should be obvious they are not credible because (A) the 44% estimate comes from case-series, and is thus heavily ascertained, and (B) the 38% estimate comes from two case-series, two case-reports, and four very unrepresentative cohort-studies (of “severe infantile autism”, kids referred for some reason for FRA testing, a sample referred for LPs, and kids with “autistic regression”).
In other words, because these are not representative cohorts of autistic kids, they cannot, except by extreme luck, indicate the prevalence in the general population.
As an aside, the mass prescription of leucovorin to autistics is going to cause harm for the fairly large (~1/6-1/5) share of autistics who suffer from seizures because leucovorin can inhibit anti-seizure medications. I hope doctors will take account of this before prescribing leucovorin haphazardly.
Notably, Baccarelli’s review relied extensively on this sort of evidence. If I had to speculate, I’d say he only saw this worth criticizing when it came to the sibling study because he didn’t want the null result to be correct.
This is your best time post I have read so far. It is well organized and introduced the topic well. Generally, I have found your time posts hard to follow.
I admire you writing this. I know your incentives would be to go along with the administration or just ignore the topic. But it is an important topic, and you are doing the right thing speaking truth.