
Could Universal GLP-1 Drugs End the Obesity Epidemic?
Studies say... yes! And it might even save households money.

If you’re looking to acquire Semaglutide, Tirzepatide, Retatrutide or other GLP-1RA drugs at an extremely low price of around $15-$40 per month, see this article.
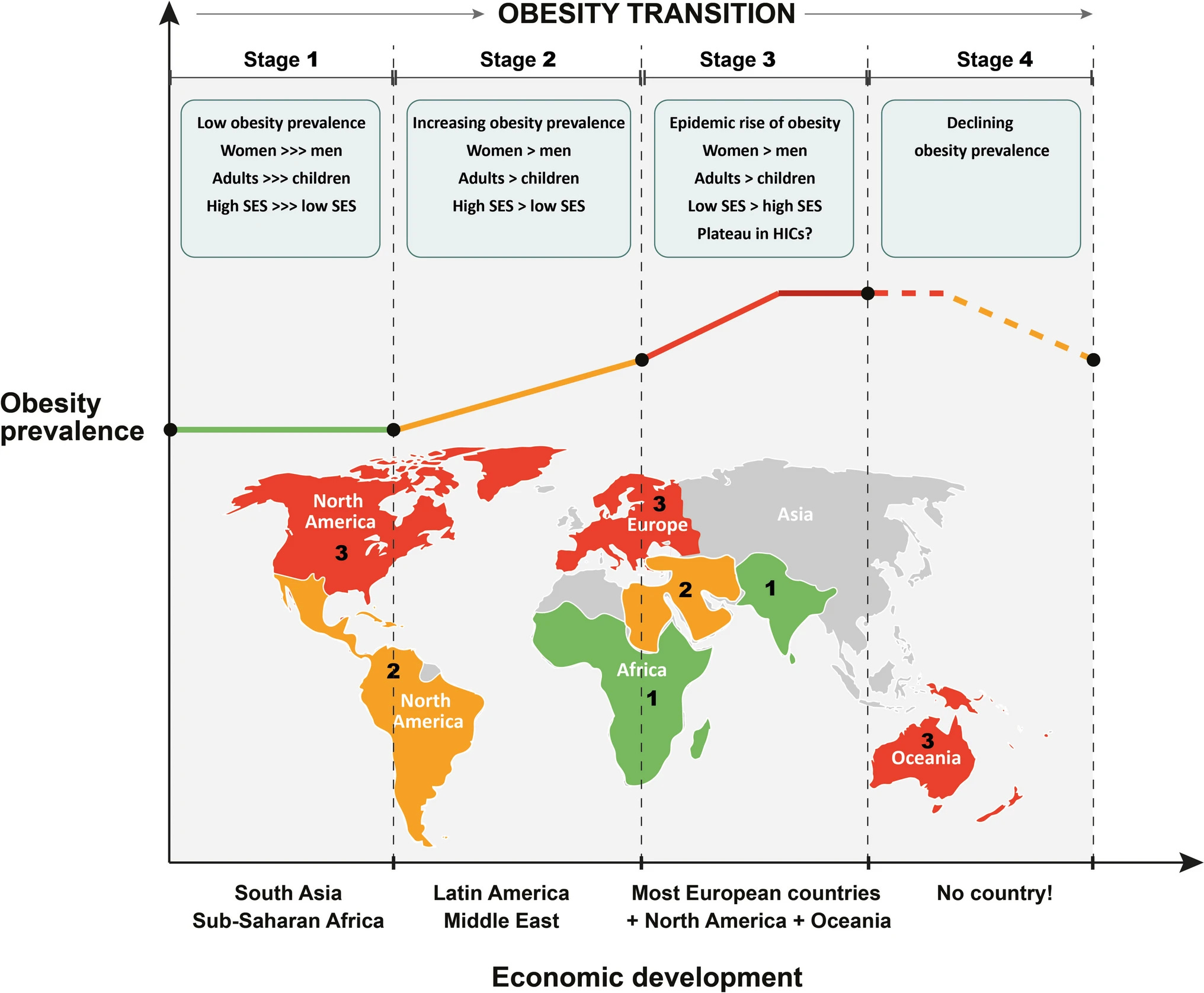
Obesity has been increasing for a very long time (not just since 1980). Given that this increase is reliably tied so countries getting wealthier, this development might be a natural part of the process of development. Similar to the demographic transition, there may also be an ‘obesity transition.’ We can see the obesity transition very clearly by looking across Latin America, where countries in different stages of development seem to be moving consistently into different transition stages.
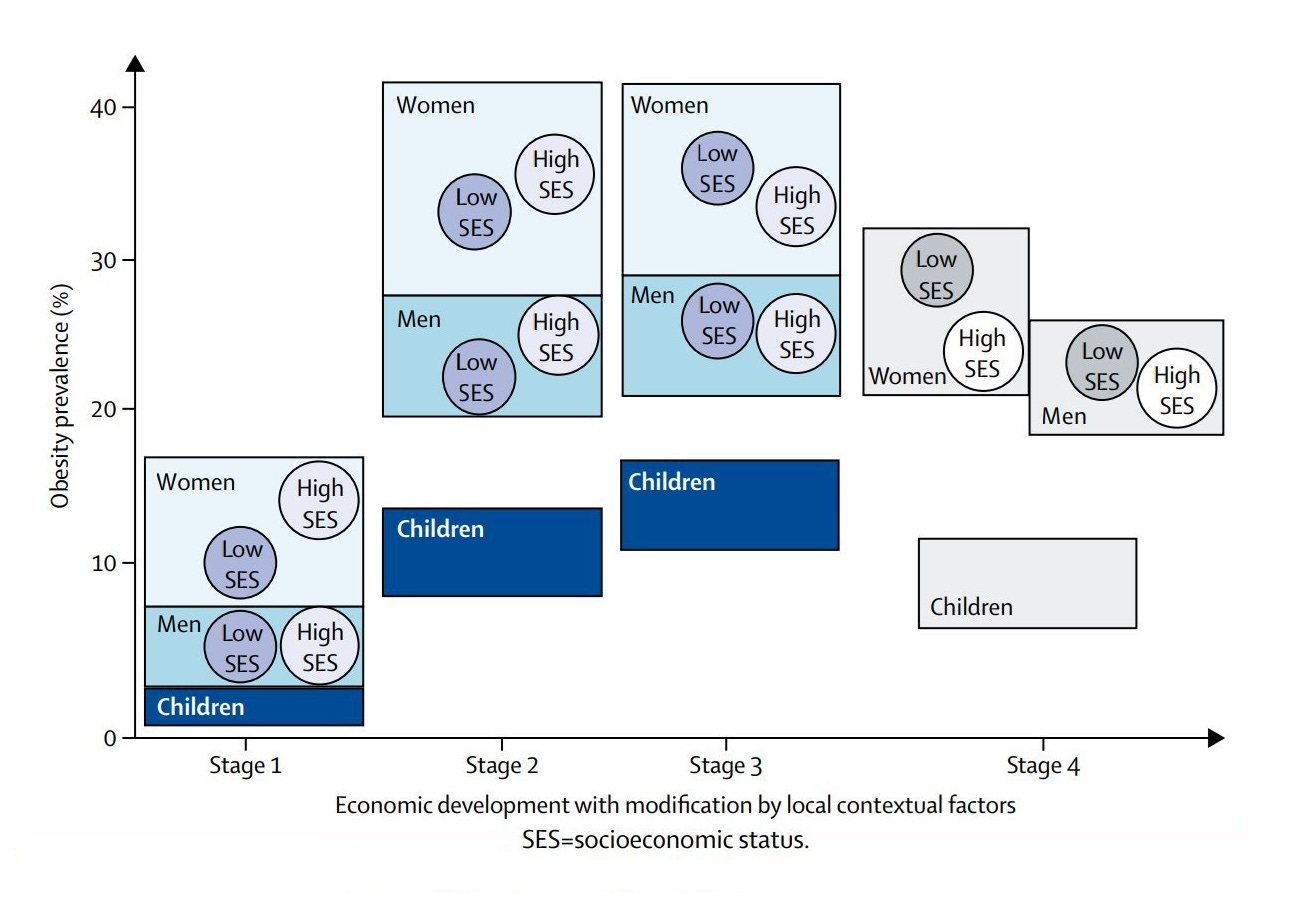
The obesity transition, through the three stages we see in today’s data, looks like this:
Or for an alternative view, consider this diagram:
The curious thing is whether there’s a fourth stage. America could be entering the fourth stage right now. Consider that for two consecutive years, obesity has been declining. Speculation about this possible fourth stage has, with good reason, focused largely on pharmacological solutions—chiefly GLP-1 receptor agonist drugs (GLP-1RAs) like Ozempic and Zepbound. But can we use technology to pop the obesity bubble? Can we ‘cure’ the obesity epidemic by getting fat people on drugs like GLP-1RAs?
Yes.
Want to skip background details and get to the results? Click here.
Obesity is defined by a BMI at or above 30. Class I obesity includes BMIs of 30-34.9, Class II ranges from 35-39.9, and Class III—Extreme Obesity—is everything at 40 or above. As an aside, when people say they’re obese but fit, they are usually wrong, but most real examples in that limited category are Class I obese. Big Ramy is one of very few people who are both fit and extremely obese. Anyway, here’s how the distributions look for men and women using the latest data from the National Health and Nutrition Examination Survey (NHANES):1
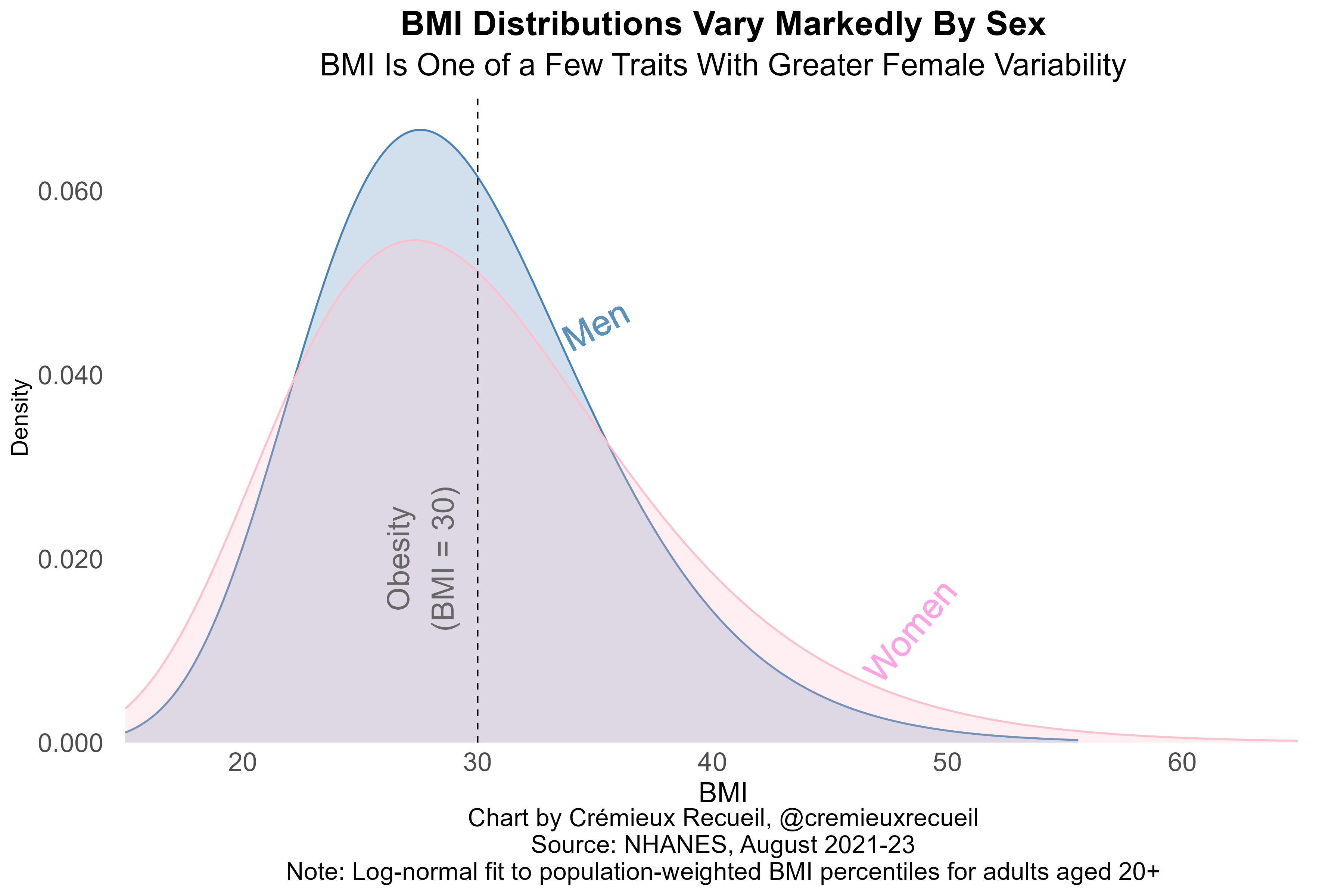
If you look at this chart or read the subtitle, you’ll notice that men are considerably less variable than women. BMI is one of the traits for which women are usually found to be more variable than men. When it comes to fat distribution, the male body plan is a lot less variable than the female one when you think about it. Think butts and boobs.
Relatedly (given the body’s resistance to losing muscle), men and women also respond to GLP-1RAs differently. In absolute terms, men tend to experience larger weight losses because they’re larger, but in relative terms, women tend to lose a larger percentage of their bodyweight when they’re on the drugs. The difference is not enormous, but we still have to keep it in mind if we’re going to correctly calculate how much GLP-1RAs could help us beat the obesity epidemic. Because we lack sex-specific numbers for retatrutide, I’m applying a constant female +2% and male -2% from overall bodyweight loss estimates across samples and when computing overall population figures, assuming that women (men) are 51% (49%) of those aged 20 plus.
The numbers I’ll use are from three trials of three different GLP-1RAs: semaglutide (active ingredient in Ozempic and Wegovy; STEP 1), tirzepatide (active ingredient in Mounjaro and Zepbound; SURMOUNT-1), and retatrutide (not yet approved; phase 2 results used). I’ll be using each trial’s interpolated or reported weight loss numbers for 52 weeks—one year—in order to figure out what obesity rates would be like after one year of universal treatment. All groups will also be matched based on their placebo group’s progress at the same time and the dosages I will be using are 2.4mg for semaglutide, 15mg for tirzepatide, and 8mg for retatrutide.
I will be assuming away a few nuisance factors. These are (1) race; (2) age; (3) current users and non-uniform effects, and; (4) diabetes status. Race and age have minimal impacts on success defined as the percentage of bodyweight lost, so I think ignoring them won’t be impactful. Diabetes status, however, has notable impacts on GLP-1RA efficacy. Namely, diabetics achieve less weight loss while on these drugs. How much less? A bit, and this applies to several non-weight loss benefits as well. Because the effect is not that large and diabetics are a minority of obese people, adjusting for their presence won’t have a large effect on results. I’ll demonstrate that below, but for now, I’ll just proceed with the numbers from the obesity trials.
I am also assuming away noise (i.e., assuming trial estimates are sufficiently accurate) and that the overweight and obese samples used in trials are similar to overweight and obese people in the real world. These assumptions are reasonable, since it seems trial samples are not that far off in weight and different similarly powered trials of comparable populations with respect to obesity produce comparable results at the same dosages of a given GLP-1RA, so it shouldn’t be an issue whether I use results from one or another of the available large-scale trials for a specific GLP-1RA.
Results are here.
If we got all the obese people on GLP-1RAs for a year, the obesity rate would fall by substantially more than half.
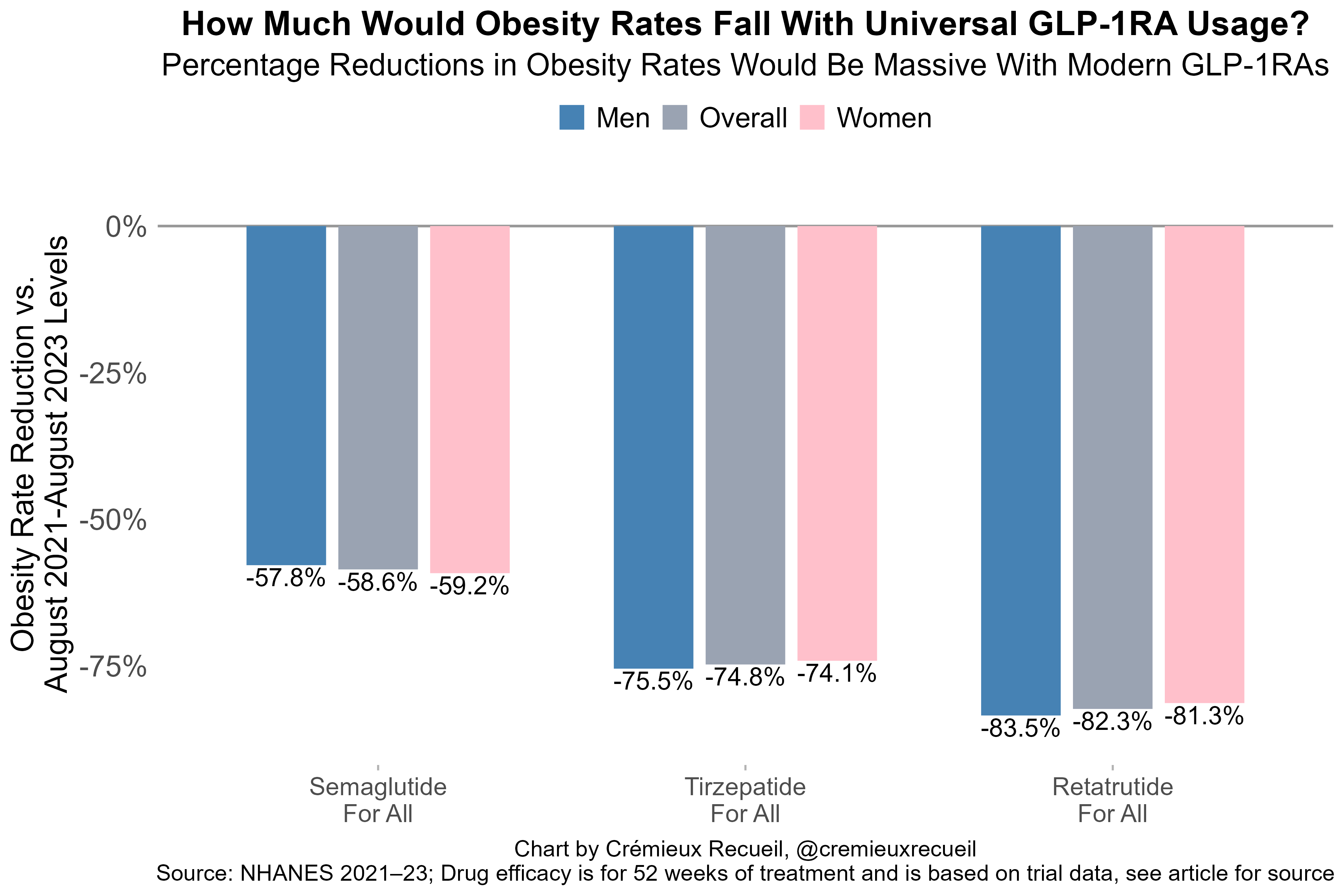
If obese people were able to and wanted to use GLP-1RAs, the obesity rate would crater. With less modern GLP-1RAs like liraglutide or dulaglutide, we likely wouldn’t see the rate decline by close to half, but with modern GLP-1RAs like semaglutide, more than half of obesity can be eliminated if they’re put to use, and this is just the efficacy for one year of use! We can take this even further.
We can technologically eviscerate the obesity rate and deliver the world from fatness.
